Refine search
Actions for selected content:
47842 results in Zoology
The association between dietary patterns and disease severity in patients with ulcerative colitis
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 10 / 28 May 2024
- Published online by Cambridge University Press:
- 02 February 2024, pp. 1803-1812
- Print publication:
- 28 May 2024
-
- Article
-
- You have access
- HTML
- Export citation
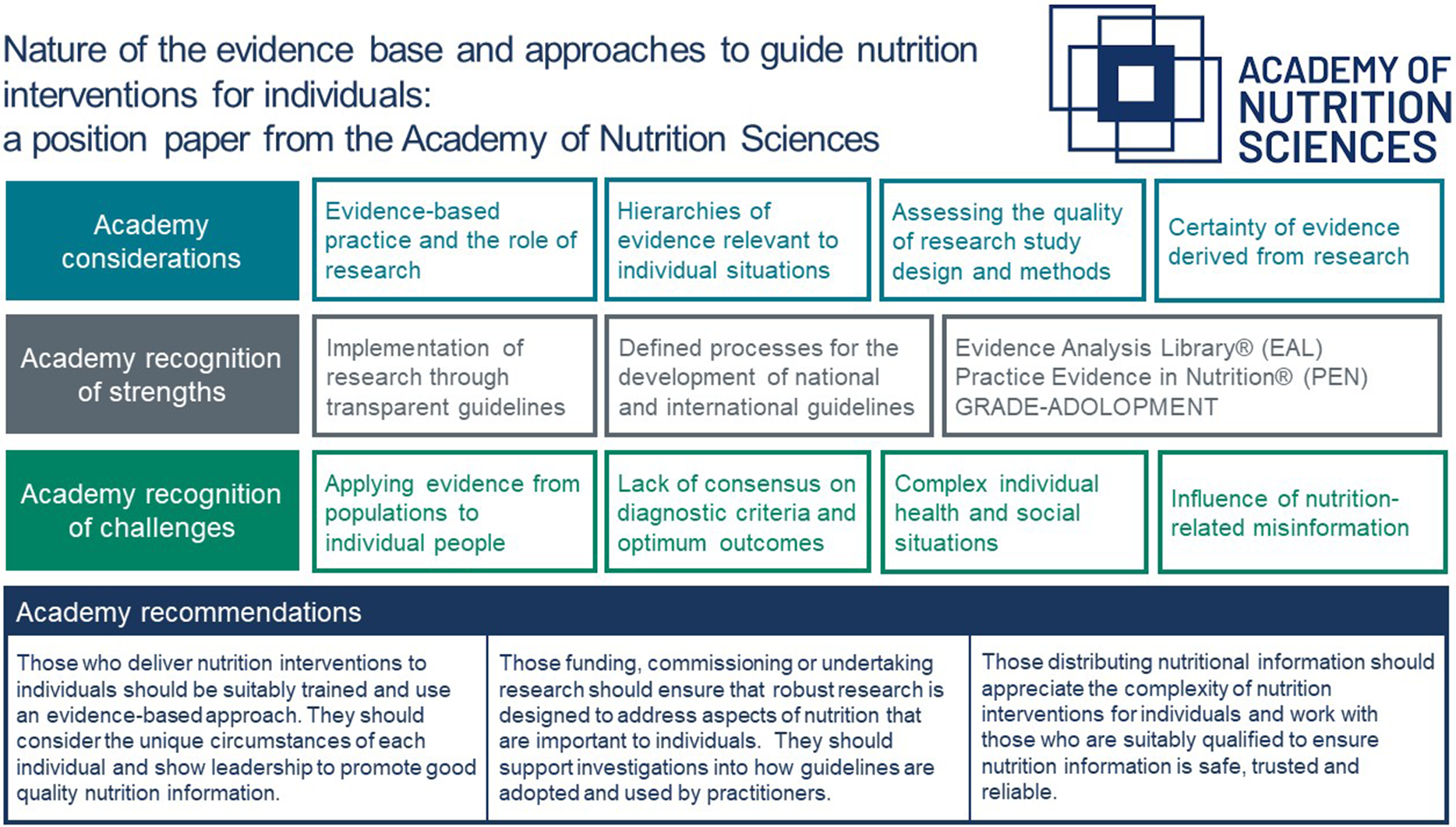
Nature of the evidence base and approaches to guide nutrition interventions for individuals: a position paper from the Academy of Nutrition Sciences
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 10 / 28 May 2024
- Published online by Cambridge University Press:
- 02 February 2024, pp. 1754-1773
- Print publication:
- 28 May 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Evaluation of three prediction formulas of 24-hour urinary sodium excretion in Chinese residents: a systematic review and meta-analysis
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 02 February 2024, e71
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Exploring the prospective acceptability of a healthy food incentive program from the perspective of people with type 2 diabetes and experiences of household food insecurity in Alberta, Canada
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 02 February 2024, e66
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Household food insecurity and physical activity behaviour in Ecuadorian children and adolescents: findings from the Ecuador 2018 National Health and Nutrition Survey (ENSANUT-2018)
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 02 February 2024, e67
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Identifying barriers and facilitators to increase fibre intakes in UK primary school children and exploring the acceptability of intervention components: a UK qualitative study
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 01 February 2024, e59
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Direct and indirect associations of experience of racial discrimination, dietary patterns and obesity in adults from southern Brazil
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 01 February 2024, e60
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Complementarity between the updated version of the front-of-pack nutrition label Nutri-Score and the food-processing NOVA classification
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 01 February 2024, e63
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
H2OAthletes study protocol: effects of hydration changes on neuromuscular function in athletes
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 9 / 14 May 2024
- Published online by Cambridge University Press:
- 01 February 2024, pp. 1579-1590
- Print publication:
- 14 May 2024
-
- Article
-
- You have access
- HTML
- Export citation
High starch intake favours body weight control in neutered and spayed cats living in homes fed ad libitum
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 10 / 28 May 2024
- Published online by Cambridge University Press:
- 31 January 2024, pp. 1786-1802
- Print publication:
- 28 May 2024
-
- Article
-
- You have access
- HTML
- Export citation
Barriers and facilitators to consuming pulses: a qualitative exploration including effects of trying recipes at home
-
- Journal:
- Journal of Nutritional Science / Volume 13 / 2024
- Published online by Cambridge University Press:
- 31 January 2024, e6
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Bridging the gap between science and food policy: nutrition as a driver of policy drawing on Scotland as a case study
- Part of
-
- Journal:
- Proceedings of the Nutrition Society / Volume 83 / Issue 3 / September 2024
- Published online by Cambridge University Press:
- 30 January 2024, pp. 204-209
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
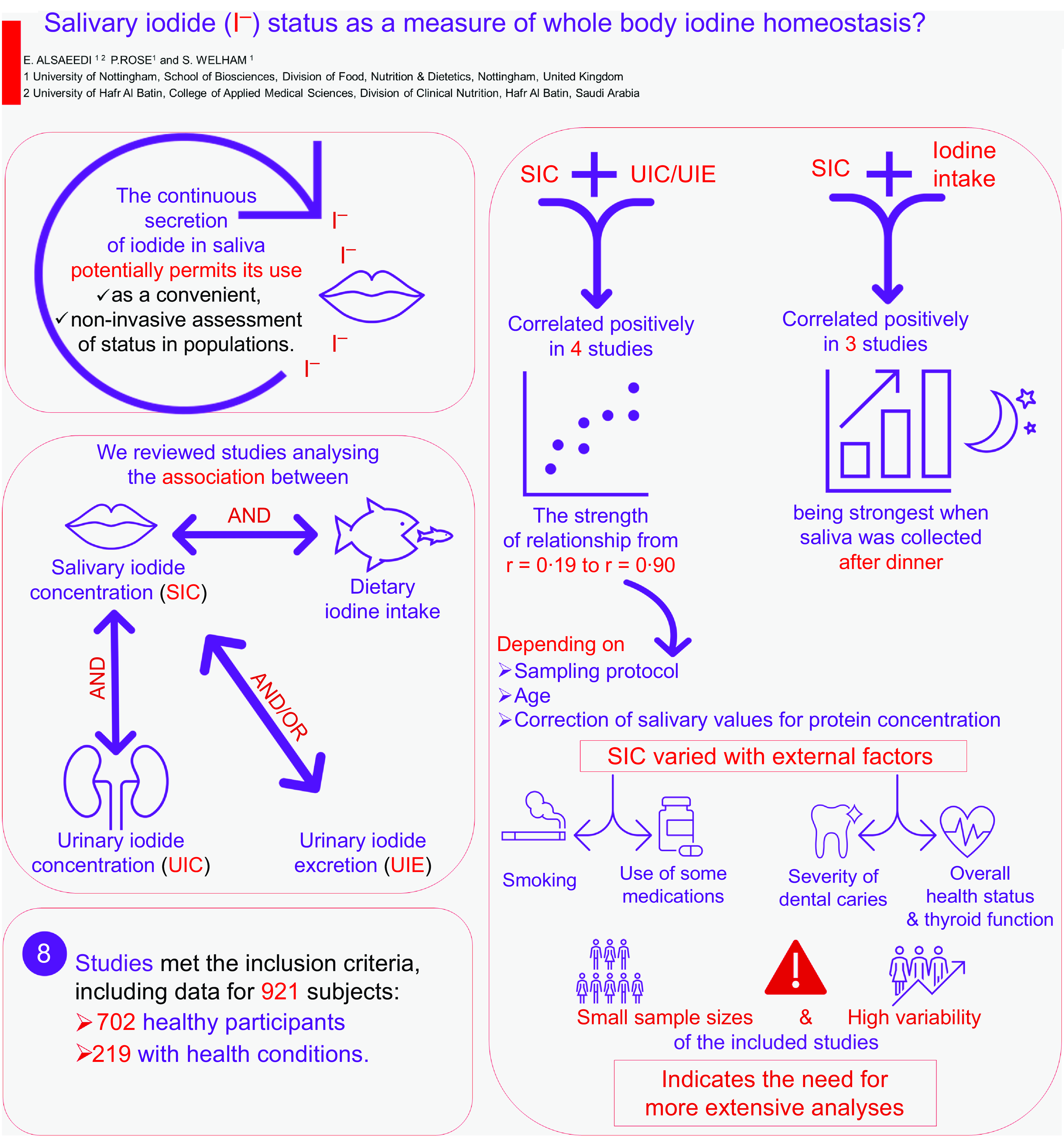
Salivary iodide status as a measure of whole body iodine homoeostasis?
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 10 / 28 May 2024
- Published online by Cambridge University Press:
- 30 January 2024, pp. 1740-1753
- Print publication:
- 28 May 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Effects of physical form of β-lactoglobulin and calcium ingestion on GLP-1 secretion, gastric emptying and energy intake in humans: a randomised crossover trial
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 10 / 28 May 2024
- Published online by Cambridge University Press:
- 30 January 2024, pp. 1730-1739
- Print publication:
- 28 May 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
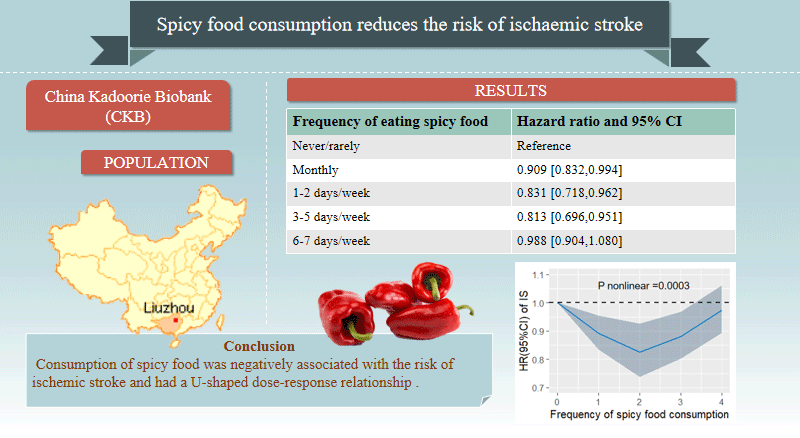
Spicy food consumption reduces the risk of ischaemic stroke: a prospective study
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 10 / 28 May 2024
- Published online by Cambridge University Press:
- 30 January 2024, pp. 1777-1785
- Print publication:
- 28 May 2024
-
- Article
-
- You have access
- HTML
- Export citation
Saturated fat and CVD: importance of inter-individual variation in the response of serum low-density lipoprotein cholesterol
- Part of
-
- Journal:
- Proceedings of the Nutrition Society / Volume 84 / Issue 1 / February 2025
- Published online by Cambridge University Press:
- 29 January 2024, pp. 87-97
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
An overview of the nutritional status of childbearing age women, children and adolescents living in a rural area of Madagascar: preliminary results of the Tany Vao project
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 29 January 2024, e52
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Association between n-3 PUFA and lung function: results from the NHANES 2007–2012 and Mendelian randomisation study
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 10 / 28 May 2024
- Published online by Cambridge University Press:
- 26 January 2024, pp. 1720-1729
- Print publication:
- 28 May 2024
-
- Article
-
- You have access
- HTML
- Export citation
Mediators and moderators of the effects of a school-based intervention on adolescents’ fruit and vegetable consumption: the HEIA study
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 25 January 2024, e50
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Impact of the dietary transition to minimise environmental impacts on micronutrient intakes: a systematic literature review
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE6 / January 2023
- Published online by Cambridge University Press:
- 25 January 2024, p. E377
-
- Article
-
- You have access
- HTML
- Export citation
