MANUSCRIPT PREPARATION
Authors are encouraged to follow the Uniform Requirements for Manuscripts Submitted to Biomedical Journals; this is the format used in PubMed/MEDLINE. They should strive for a concise article that is unencumbered by excessive detail. Authors who are not fluent in English should have their manuscript checked by a native speaker of English and/or an editing service that provides such assistance. Manuscripts that do not follow the required format or are poorly prepared may be rejected for that reason.
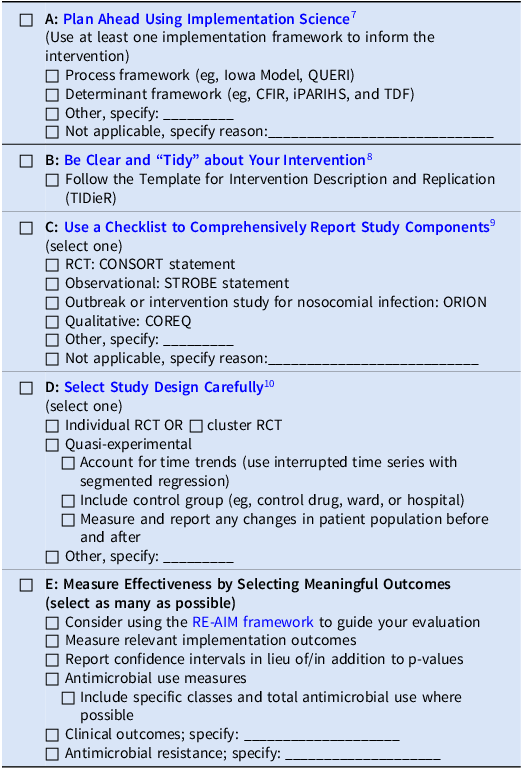
For guidance regarding the reporting of randomized (CONSORT), observational (STROBE), meta-analyses (PRISMA), and other clinical trials, please consult www.equator-network.org. For recommendations regarding the design and analysis of antimicrobial stewardship intervention studies, please review the 5 Steps to High Quality Antimicrobial Stewardship Research. Authors are encouraged to complete the checklist A Simple Blueprint for Antimicrobial Stewardship Intervention Research. Double space the entire manuscript, including title page, abstract, body, references, tables, and figure legends. Use left justification only, so that the right margin is ragged. Number pages consecutively, beginning with the title page. Use a standard font (such as Times New Roman or Helvetica) and set the font size to 12 points (for tables as well as text). Each component of the article should begin on a separate page, as follows: title page, abstract, body text, acknowledgments, references, appendices, figure legends, and tables. All these components must be in a single file, except any figures, each of which should be a separate file (see Figures and Figure Legends, below).
For revised submissions please upload both a clean version of the revised manuscript and a version with changes marked, either with tracked changes or highlighted.
Title Page
The title page should include the following information: (1) the title of the manuscript; (2) the names of the author(s), including each author's highest academic degree or professional certification; (3) the departmental and institutional affiliation of each author, including city, state, and country; (4) the name, address, telephone number, fax number, and e-mail address of the author responsible for correspondence; (5) if relevant, a statement about any previous presentation of the data or findings in a preliminary report or abstract; (6) an abbreviated title of not more than 45 characters (including spaces), to be used for search results online; and (7) a word count for the body of the text (i.e., excluding the abstract and the references). Acknowledgment of financial support and potential conflicts of interest must be included and should be placed in the Acknowledgments section (see below).
Abbreviations should conform to those given in the AMA Manual of Style. Symbols for units of measurement (mm, mL) should not be followed by periods. Chemical or generic names of drugs, materials, and equipment are strongly preferred; a proprietary name may be given only after it is preceded by the generic or chemical name the first time it appears and must be followed by the name of the manufacturer or supplier. Terms and abbreviations must be defined at first use, separately for the abstract, the body, and each table and figure. Use only common abbreviations and use as few as possible; and do not abbreviate terms used fewer than 5 times. Abbreviate genus names after first mention.
Abstract. Original Articles should include a structured abstract of no more than 250 words. The following headings are suggested: Objective, Design, Setting, Patients (or Participants), Methods (or Interventions), Results, and Conclusions. If this list of headings is inappropriate, variations are permitted: for example, a study that involved no intervention would use the heading "Methods" rather than "Intervention"; or an analysis of an existing data set might use the heading "Methods" in place of both "Intervention" and "Setting." For brevity, parts of the abstract can be written in phrases rather than complete sentences, .e.g.,"Design: Retrospective cohort study". The contents of each section should conform to the guidelines below.
Objective. Begin with a clear statement of the precise objective or question addressed in the report. If more than one objective is addressed, indicate the main objective and state only key secondary objectives. If an a priori hypothesis was tested, it should be stated.
Design. Describe the basic design of the study. Include the duration of follow-up, if any. Use as many of the following terms as apply.
- For intervention studies: randomized controlled trial; nonrandomized controlled trial; double-blind; placebo controlled; crossover trial; before-after trial.
- For studies of screening and diagnostic tests: indicate the criterion standard against which a new or alternative test is being compared; blinded or masked comparison.
- For studies of prognosis: inception cohort (subjects assembled at a similar and early time in the course of the disorder and followed thereafter); cohort (subjects followed forward in time, but not necessarily from a common starting point); validation cohort or validation sample, if the study involves the modeling of clinical predictions.
- For studies of causation: randomized controlled trial; cohort; case-control; survey (preferred to "cross-sectional study").
- For descriptions of the clinical features of medical disorders: survey; case series.
- For studies that include a formal economic evaluation: cost-effectiveness analysis; cost-utility analysis; cost-benefit analysis. For new analyses of existing data sets, the data set should be named and the basic study design disclosed.
Setting. To assist readers in determining the applicability of the report to their own clinical circumstances, include a brief description of the study setting(s) such as: primary or tertiary referral center, private or public institution, or an ambulatory or acute care setting.
Patients or participants. Provide information on important eligibility criteria, and key sociodemographic features of patients and how they were selected, including the number of otherwise eligible subjects who were approached but refused to participate. If matching was used for comparison groups, specify the characteristics that were matched. In follow-up studies, the proportion of participants who completed the study must be indicated. In intervention studies, the number of patients withdrawn because of adverse effects should be given.
For selection procedures, these terms should be used, if appropriate: random sample ("random" refers to a formal, randomized selection in which all eligible subjects have a fixed and usually equal chance of selection); population-based sample; referred sample; consecutive sample; volunteer sample; convenience sample.
Intervention(s). Describe the essential features of any interventions, including the method and duration of administration. The intervention should be named by its most common clinical name (eg, the generic term "oseltamivir"), the brand name of a drug, if a specific product was studied, and the name of the manufacturer or supplier for any product(s) mentioned in the manuscript, including software.
Results. Give the main results of the study in narrative form. Define measurements that require explanation for the expected audience of the manuscript. If possible, the results should be accompanied by objective data and the exact level of statistical significance. For comparative studies, confidence intervals should relate to the differences between groups. When risk changes or effect sizes are given, indicate absolute values, so that the reader can determine the absolute, as well as relative, impact of the finding. Approaches such as "number needed to treat" to achieve a unit of benefit are encouraged when appropriate. Studies of screening and diagnostic tests should use the terms sensitivity, specificity, and likelihood ratio. If predictive values or accuracy are given, prevalence or pretest likelihood should be given as well.
Conclusions. Only those conclusions of the study that are directly supported by the evidence reported should be given, along with the clinical application; indicate whether additional study is required before the information should be used in normal clinical settings. Equal emphasis must be given to positive and negative findings of equal scientific merit.
Clinical trials identifier. If your manuscript is the report of a randomized clinical trial that has been registered in a public trials registry, please provide the trial registry name, the registration identification number, and the URL for the registry at the end of the abstract. This information will be published in the journal if the manuscript is accepted.
Body Text
The main sections and subdivisions of the body text should be indicated by side heads flush with the left margin and two lines above the text.
Keep Introduction, Methods, Results, and Discussion distinct and separate. The Methods section should provide detail sufficient to allow others to re-create your experiment. Methods may not be described or restated in figure legends or table notes, but must be all together in the Methods section. The Results section contains the previously unpublished data derived by this application of your methods. The Discussion section contains your interpretation of the reported data and comments on its meaning. There should be no separate section labeled "Conclusion." Avoid duplicating in the text data that have been provided in tables or figures. Also avoid duplication within the text; the Discussion section should not restate all the findings that have been presented in Results and/or in tables and figures.
The Editor requests that authors reporting the results of clinical trials describe clearly the following: (1) eligibility criteria; (2) whether subjects were admitted before allocation to one of the study groups; (3) the method of randomization; (4) whether the study was "masked," what specific information was masked, and whether subjects, clinicians, and evaluators were masked; (5) the method used to identify treatment complications; (6) an explanation and analysis of subjects lost to follow-up; (7) statistical methods used; and (8) information that led to the determination of the size of the study groups and the expected differences between groups. For all studies involving human or animal subjects, the Methods section should include a statement that the study was reviewed and approved by the authors' institutional review board. Informed consent must be obtained for all study participants. Footnotes are acceptable in tables but cannot be used in the body of the manuscript; any footnotes in your manuscript will be integrated into the text, perhaps in parentheses.
Required Statements
The below listed sections must be included, with the exception of Author Contributions, which is considered optional. Please check you have included all of these statements at the end of the manuscript, before the References section.
1. Acknowledgements. You may acknowledge individuals or organizations that provided advice, support (non-financial). Formal financial support and funding should be listed in the Financial Support section (see below).
Persons should not be thanked in the Acknowledgments section without their knowledge and consent. Authors will be asked during the submission process to confirm they obtained permission from all persons thanked by name in the Acknowledgments section.
Authorship and manuscript preparation. If the manufacturer of a product discussed in a submitted manuscript had a role, either directly or through a third party, in the gathering or preparation of data or in the writing of the manuscript, that information must be disclosed in the Acknowledgments section. If anyone other than the named authors had a role in the gathering or preparation of data or in the writing of the manuscript, that too should be disclosed. Examples:
- Manuscript preparation. Steris Corporation provided assistance with study design and data acquisition.
- Manuscript preparation. Statistical and other analyses were done by 3M Medical Division.
- Manuscript preparation. MedCommunications (Philadelphia) provided assistance in preparing and editing the manuscript.
2. Author Contributions. In the process of submitting an article to ASHE, the corresponding author is prompted to provide further details about contributions to the article using the CRediT taxonomy. People who have contributed to the article but do not meet the full criteria for authorship should be recognized in the acknowledgements section; their contribution can also be described in terms of the CRediT taxonomy. This section is optional.
3. Financial support. The Financial Support statement should list all sources of financial support for the work, including any financial arrangement with a company whose product is related to the study. If there was no financial support, that too should be stated. The statement should be consistent with disclosures that would be stated in the ICMJE Form for Disclosure of Potential Conflicts of Interest.
Examples:
- Financial support. The GERES Project is supported by the French Ministry of Health. Additional support for this study was provided by Becton-Dickinson and SIMS France.
- Financial support. H.S.C. received grant support from the Department of Veterans Affairs Rehabilitation Research and Development Service Merit Review (C2234-MD and C3-2442MD), D.B.L. received support from the US Public Health Service (grant HC41024), and A.E.T. received salary support from an Emerging Infectious Diseases Cooperative Agreement. C.U. receives 2% salary support from Aventis Pasteur for work on another study.
- Financial support. None reported.
4. Conflict of interest. Conflicts of Interest are situations that could be perceived to exert an undue influence on an author’s presentation of their work. They may include, but are not limited to, financial, professional, contractual or personal relationships or situations. Conflicts of Interest do not necessarily mean that an author’s work has been compromised. Authors should declare any real or perceived Conflicts of Interest in order to be transparent about the context of their work.
The conflict of interest statement must contain a statement of potential conflicts of interest. If the manuscript is accepted for publication, the disclosures will be published. The Acknowledgments section of the manuscript must list the name of each contributing author and any potential conflicts of interest for each author for the previous three years; if no potential conflict exists, that too should be stated. The statement should be consistent with disclosures that would be stated in the ICMJE Disclosure Form. There is a potential conflict of interest when anyone involved in the publication process has a financial or other beneficial interest in the products or concepts mentioned in a submitted manuscript, or in competing products, that might bias his or her judgment. Examples of potential conflicts of interest with respect to a company whose product is mentioned in the manuscript include owning stock (except as part of a diversified portfolio), receiving grants, serving as a consultant, or being on the speakers' bureau. (This information is exclusive of the financial support discussed above.)
Examples:
- Potential conflicts of interest. S.A. and K.H. report that they are shareholders in Loke Diagnostics (Aarhus, Denmark).
- Potential conflicts of interest. K.L.H. reports having consulted for and having received grant support from Astellas and reports having received an honorarium from Cubist before starting employment with the New York Department of Public Health in 2009.
- Potential conflicts of interest. E.F.M. reports that she has been a consultant to Merck, Novartis, and GlaxoSmithKline and is member of the speakers' bureaus for Ortho McNeil and Novartis. J.A.S. reports that he received research funding from Bayer and Ortho McNeil and that he has been a consultant for Bayer and Pfizer. J.D.C. reports that he is an employee of AB Biodisk.
- Potential conflicts of interest. All authors report no conflicts of interest relevant to this article.
Disclosure documentation. All authors of Original Articles, Concise Communications, and Research Briefs are required to complete and upload the ICMJE Form for Disclosure of Potential Conflicts of Interest when and if they are asked to submit a revision of their manuscript. All authors of Letters and invited manuscripts (Letters in Reply, Commentaries, Reviews, and Guidelines) are required to complete and upload the ICMJE Disclosure Form when they initially submit their manuscript. Note that this documentation is in addition to the disclosure statements in the Conflict of Interest section of the manuscript file.
5. Research Transparency and Reproducibility. A data availability statement should be included and provide URLs for any available datasets or code.
In the interests of supporting transparency and openness, when possible, authors should make available any data sets, code, materials, processes, and any other resources that would be necessary for others to fully evaluate the basis for any findings, and to verify or reproduce the work. Authors should include any information that will be required by others to allow them to access, interpret and process these resources.
When possible, ASHE recommends that resources be made publicly available via repositories that:
- Are supported and recognized by the community as appropriate for the resources they hold.
- Provide stable, unique identifiers for the information they hold.
- Support linking between their database records and associated published research articles.
- Allow free public access to their holdings, with reasonable exceptions (such as administration charges for the distribution of physical materials).
Examples of general repositories include Dryad, Zenodo, Figshare, Dataverse and the Open Science Framework.
For information about citing external data, please take a look at IASSIST’s Quick Guide to Data Citation.
{kind=link}