HIV-positive patients with schizophrenia spectrum disorders experience burden of double stigma. Comorbid pathology may alter structure of stigma and shall be considered in development of individual destigmatization programs.
Study of psychiatric stigma features in HIV-positive and HIV-negative patients with schizophrenic disorders.
ISMI (Ritsher et al., 2003), PDD (Link et al., 1991) – to study stigma in 70 patients divided into three groups with respect to their diagnosis (I — F20.x, II — F21.x, III— F2x+HIV); BPRS (Overall & Gorham, 1962) – to assess psychiatric status, RSAS (Eckblad et al., 1982) – to assess anhedonia. Dispersion analysis (Kruskal and Mann–Whitney tests), Spearman and Pearson correlation were used.
Patients with comorbid HIV-infection showed increased level of perceived stigma, although they resisted the stigma internalization better than others did (Table 1).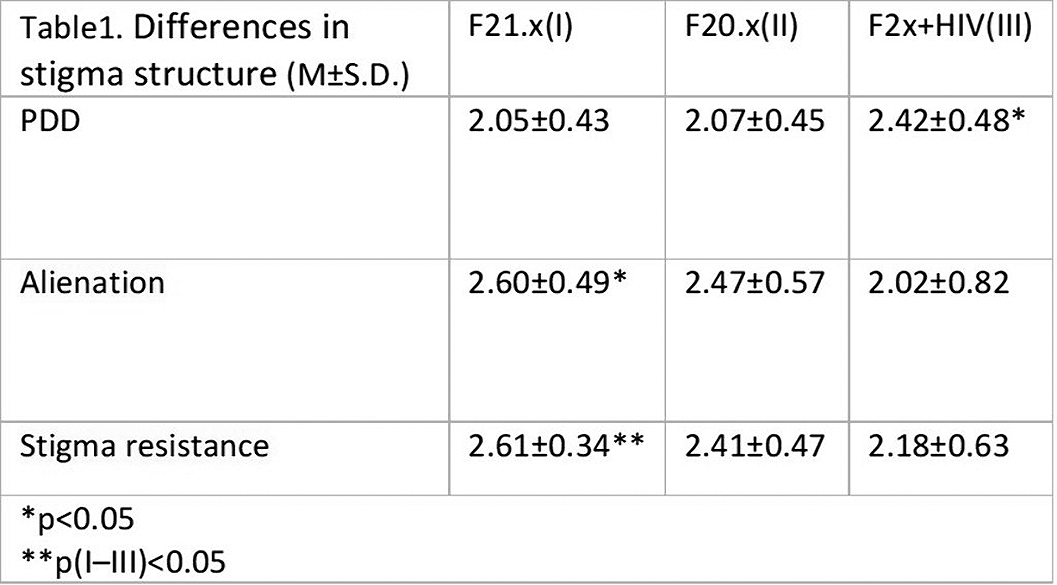
Patients with schizotypal disorders and patients at early stages of HIV infection experienced the most alienation and frailty to internalization of stigma (Tables 1, 2).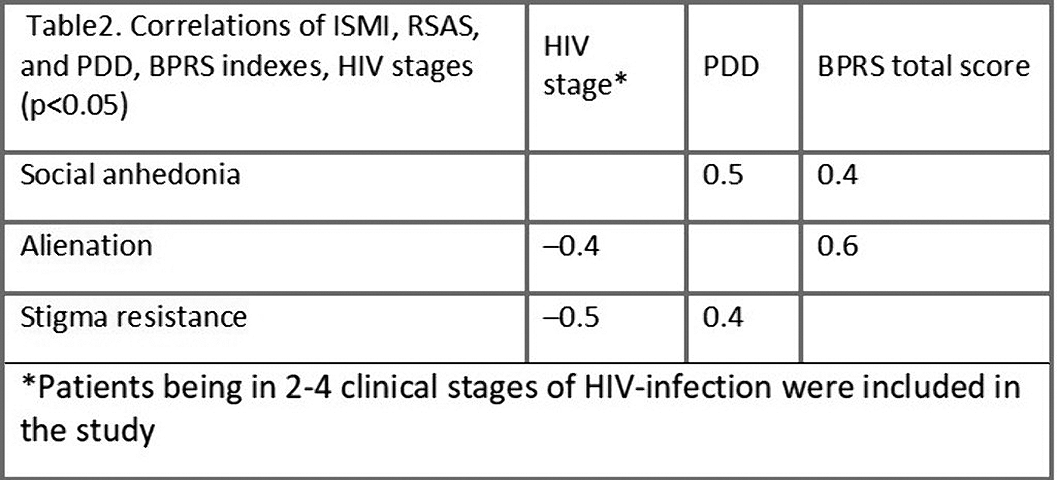
Correlation relationship between social anhedonia and perceived stigma (r=0.5, p<0.05) observed in patients with HIV infection.
Comorbid HIV infection in psychiatric patients contributes to the psychiatric stigma structure. Differentiated approaches in rehabilitation of HIV-positive mental patients should be used.

