


Most children and adolescents living in the USA consume less than the recommended daily amounts of fruits, vegetables, whole grains and dairy products(1,Reference Liu, Rehm and Onopa2) . Such deviations from dietary guidelines are associated with poorer health outcomes throughout the lifespan. Diet and diet-related chronic diseases, including heart disease, diabetes and chronic kidney disease, rank among the top causes of disability and death in the USA(Reference Mokdad, Ballestros and Echko3), and substandard dietary intake is the leading cause of death globally(Reference Afshin, Sur and Fay4).
Preparing and consuming home-cooked meals, as opposed to eating meals prepared outside the home, have been associated with healthier diet quality including consumption of less total calories, carbohydrates, fat and sugar(Reference Wolfson and Bleich5) and more servings of fruits and vegetables(Reference Tiwari, Aggarwal and Tang6). Unfortunately, the USA has experienced a cultural shift away from cooking and eating at home. People devote about half as much time to cooking each day compared to 50 years ago and spend more than half of their food budget on foods eaten away from home(Reference Stewart, Lusk, Roosen and Shogren7). Diet quality has likely been impacted by these changes, as foods eaten away from home generally contain more fat, sugar and salt than home-cooked alternatives(Reference Mills, Brown and Wrieden8).
Cooking and nutrition programmes have emerged as a strategy to improve diet quality through hands-on culinary instruction paired with nutrition education(Reference Asher, Shrewsbury and Bucher9). Beyond teaching culinary skills, these programmes aim to improve food literacy, defined as ‘the knowledge, skills, and behaviours needed to incorporate healthy food into one’s diet to promote lifelong wellbeing’(Reference Vidgen and Gallegos10–Reference Condrasky and Hegler12). Youth culinary and nutrition programmes have gained popularity in part because of the preventive role food literacy education may play in reducing childhood obesity(Reference Nelson, Corbin and Nickols-Richardson11,Reference Utter, Denny and Lucassen13) . Although healthy cooking programmes vary in scope and duration, even short-term exposure has been shown to positively influence youth cooking skills(Reference Saxe-Custack, Lofton and Hanna-Attisha14,Reference Hersch, Perdue and Ambroz15) , cooking attitudes(Reference Saxe-Custack, LaChance and Hanna-Attisha16,Reference Hasan, Thompson and Almasri17) , diet quality(Reference Utter, Denny and Lucassen13,Reference Saxe-Custack, LaChance and Hanna-Attisha16–Reference Vaughan, Cade and Hetherington18) and health-related quality of life(Reference Saxe-Custack, LaChance and Hanna-Attisha16).
In recent years, a number of in-person cooking programmes have expanded their reach by launching virtual versions. While some programmes use recorded video lessons to instruct participants(Reference Herman, Kimmel and Shodahl19,Reference Murad, Alford and Davis20) , other virtual classes connect programme staff and participants via an interactive livestream where instructors and participants cook together(Reference Soltanmammedova, Harner and Hornbeck21–Reference Saxe-Custack and Egan26). The virtual format requires that all participating households be equipped with the necessary food items and cooking tools to make the class recipes, and participants are generally responsible for acquiring these items on their own(Reference Herman, Kimmel and Shodahl19,Reference Murad, Alford and Davis20,Reference Doxey, Wolferz and Stewart22–Reference Sommer, Pelletier and Roche24) . Participants must have Internet access and appropriate technology, such as a laptop, tablet or cell phone, to engage with the virtual lessons(Reference Herman, Kimmel and Shodahl19,Reference Murad, Alford and Davis20,Reference Doxey, Wolferz and Stewart22–Reference Sommer, Pelletier and Roche24) .
Many virtual cooking programmes were launched in the USA during the COVID-19 pandemic when individuals and families were spending most of their time at home(Reference Herman, Kimmel and Shodahl19–Reference Patrick, Henkhaus and Zickafoose28). Preliminary results have suggested that participation in virtual cooking programmes is associated with improvements in cooking attitudes(Reference Soltanmammedova, Harner and Hornbeck21,Reference Sommer, Pelletier and Roche24) and skills(Reference Herman, Kimmel and Shodahl19–Reference Doxey, Wolferz and Stewart22,Reference Saxe-Custack and Egan26) . However, little is known about participant experiences with these programmes as well as their perceived impact on individuals and households. This study sought to elucidate perceptions of a virtual cooking and nutrition programme, Flint Families Cook, to understand family experiences.
Methods
Study design
This study, guided by Social Cognitive Theory, utilised reflexive thematic analysis(Reference Braun and Clarke29) to examine perceptions of and experiences with a virtual cooking and nutrition programme for youth and families. The researchers took an interpretivist theoretical perspective in order to capture participant knowledge formed through their social interactions both inside and outside of Flint Families Cook. Researchers assumed a subjective, social constructionist epistemological position that allowed participants and researchers to create knowledge together, participants through sharing their lived experiences and researchers through their interpretation of participant experiences(Reference Palermo, Reidlinger and Rees30). Researchers conducted focus groups with programme participants to collect rich, open-ended data from individuals that engaged in Flint Families Cook together, allowing for researchers to hear individual perspectives as well as shared group experiences.
Study setting
The current study was implemented in Flint, Michigan, a low-income urban area where approximately 59 % of children live in poverty(31), and a dearth of full-service grocery stores limits access to healthy, fresh, affordable foods(Reference Saxe-Custack, Lofton and Hanna-Attisha14,Reference Sadler32) . In March 2020, the surging COVID-19 pandemic presented additional challenges to those living in Flint and surrounding Genesee County. Unemployment rates in Flint swelled from 5·4 % to 29·7 % from March to April 2020(33), and food insecurity in Genesee County rose to 16 % (exceeding the 11·5 % food insecurity rate in the state of Michigan(34)). Further complicating food acquisition efforts, residents of Genesee County reported limited selection of foods and inflated prices at grocery stores during the pandemic(Reference Saxe-Custack, Lofton and Dawson35).
Flint Families Cook
Flint Kids Cook, a healthy in-person cooking and nutrition programme for youth taught in a farmers’ market kitchen, was introduced in Flint in 2017. The programme, which is described in a previous publication(Reference Saxe-Custack, LaChance and Hanna-Attisha16), was grounded in Social Cognitive Theory and included six consecutive weeks of instruction with recipes and nutrition content highlighting a specific food group. Flint Kids Cook had several active classes underway in March 2020 when the COVID-19 pandemic caused an abrupt halt to all in-person programming. Driven by the growing number of youth on the class waitlist as well as a newfound desire for child-friendly at-home activities(Reference Saxe-Custack, Lofton and Dawson35), researchers developed Flint Families Cook, a virtual cooking and nutrition programme for families(Reference Saxe-Custack and Egan26). Flint Families Cook was modelled after the in-person programme and included 7·5 h of live video instruction from a chef and registered dietitian over five consecutive weeks. From October 2020 through February 2022, a credentialed chef taught healthy recipes from a demonstration kitchen while families followed along from home. Recipe ingredients were delivered to families before class each week by a local food hub (Flint Fresh). A registered dietitian led nutrition activities that highlighted food groups included in recipes. Recipe ingredients, delivery and the 5-week course were free to participants.
Recruitment and data collection
Families were eligible to participate in Flint Families Cook if there were children in the home between the ages of 8 and 18 years. Family members were also required to speak English, have access to the Internet and a device to join the virtual classroom (such as a laptop, iPad or cell phone) and live in Flint or the surrounding area. Researchers invited all families who completed Flint Families Cook to join virtual focus group discussions which occurred 1 week after the classes had ended (week 6).
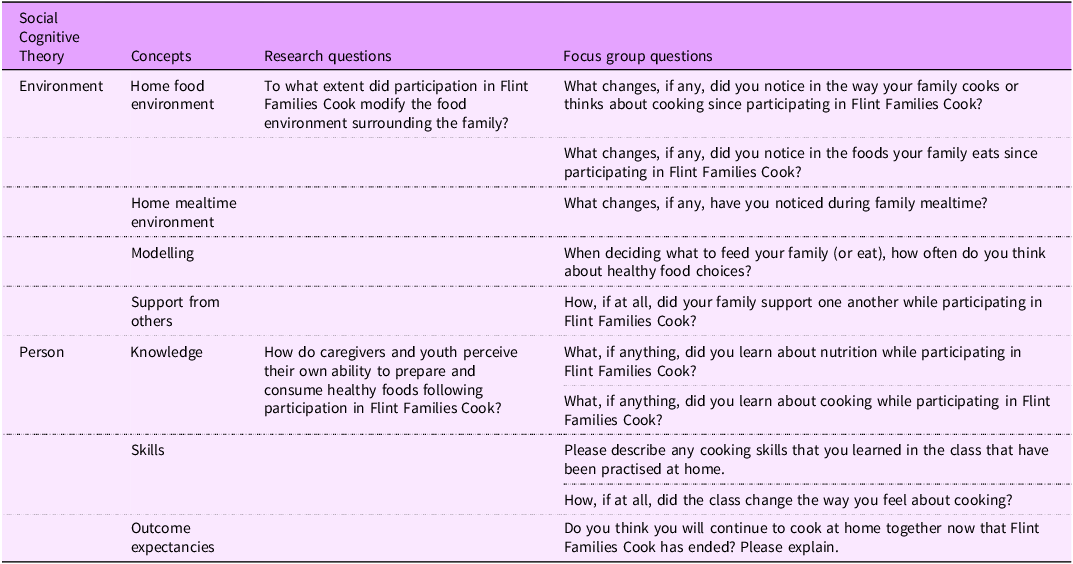
Researchers utilised the tenets and constructs of Social Cognitive Theory(Reference Bandura36) to develop the focus group guide which explored family experiences with Flint Families Cook as well as dietary behaviours and meal preparation within the home food environment (Table 1). Between November 2020 and February 2022, two researchers trained in qualitative research methods facilitated seventeen focus groups. Three focus groups were co-moderated by both researchers at the beginning of the study, and the remaining groups were moderated by one researcher while a meeting host took notes and audio- and video-recorded the session. After facilitating, moderators debriefed with the researchers who developed this paper. Each focus group included a combination of caregivers and children, with some households represented by only one caregiver or one child and other households having a combination of adults and children together, allowing researchers to explore various perspectives. Both children and caregivers contributed meaningfully to discussions. Children primarily spoke about their experiences during the class, while adults offered insights about class logistics and broader impacts of the class within the home. Focus group discussions lasted approximately 60 min, and families received one $30 gift card for their participation. Researchers concluded data collection when no new responses were offered, and data saturation had been reached. This study received exempt status from the Michigan State University Institutional Review Board. Caregivers provided written consent through a secure digital platform prior to participating in Flint Families Cook, agreeing to take part in the class and share their opinions and experiences upon completion of the programme. Likewise, children provided written assent to participate.
Table 1. Relationship between Social Cognitive Theory, concepts and questions

Data analysis
Reflexive thematic analysis was used to analyse the focus group data. Focus group discussions were transcribed verbatim. Two researchers followed a multi-phase inductive analysis process to develop meaning from the dataset(Reference Braun and Clarke29). After familiarising themselves with the data, the researchers independently coded the data and used code labels to generate initial themes that were representative of core ideas in the dataset. Together they consolidated their initially generated themes to develop themes and sub-themes that highlighted key patterns found in the dataset that were relevant to the research question. They returned to the transcripts to refine the themes and sub-themes until they felt true to the dataset. Lastly, researchers selected illustrative quotes to support each theme and sub-theme and wrote up the analysis.
Reflexivity
The authors were mindful to practise reflexivity through ongoing collaboration, returning to the dataset throughout the process to check that the analysis faithfully represented the transcripts and addressed the research questions. Authors immersed themselves in the data to interpret patterns beyond the explicit responses to the focus group questions.
Results
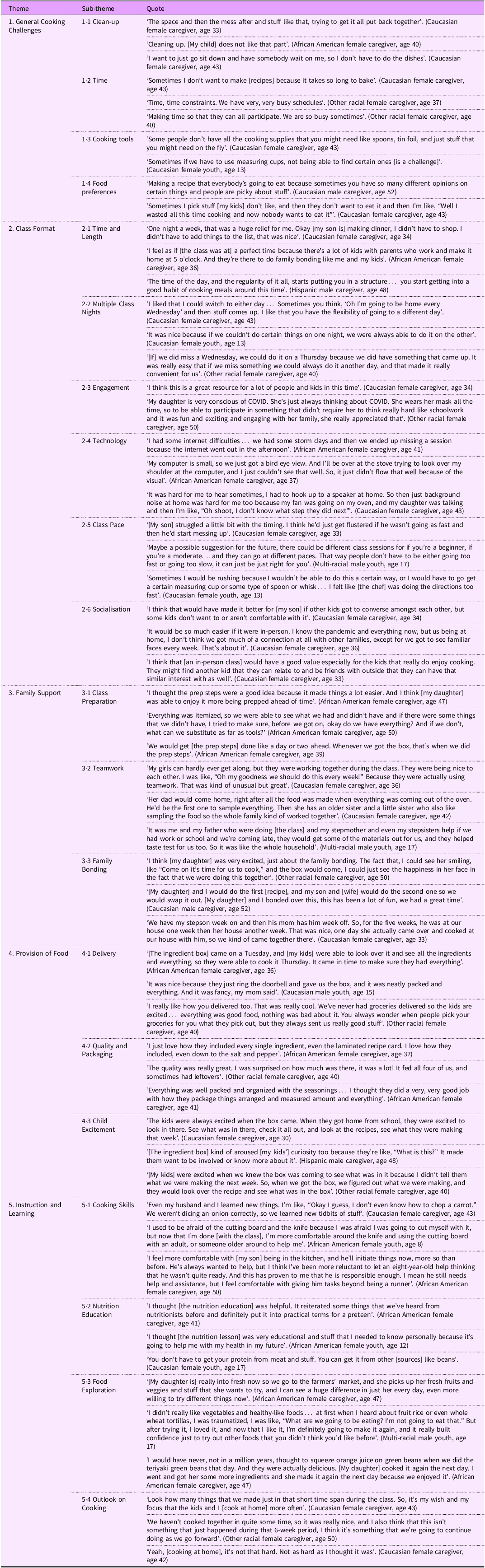
Between October 2020 and February 2022, 153 youth (mean age 11·28 ± 2·36 years) from 104 families participated in Flint Families Cook. The majority of youth identified as female (58 %), African American (69 %) and residents of Flint (75 %). A total of sixty-three participants (thirty-one adults and thirty-two youth) engaged in seventeen virtual focus groups. Similar to programme participants, the majority of youth who participated in focus group discussions identified as female (59 %), African American (53 %) and residents of Flint (81 %). Among adult focus group participants, most identified as female (90 %) and lived in Flint (71 %). Approximately 39 % identified as African American and 39 % identified as Caucasian. Five themes were generated from the focus group discussions: (i) general cooking challenges; (ii) class format; (iii) family support; (iv) provision of food; and (v) instruction and learning (Table 2).
Table 2. Illustrative quotes collected from Flint Families Cook participants

Theme 1. General cooking challenges
Many caregivers discussed general barriers that prevented regular meal preparation at home. Even among a population interested in cooking, focus group families spoke about important factors that hindered their ability or desire to cook at home. Some of these challenges included lack of time or motivation to cook, while others were related to a limited supply of cooking utensils in the home.
Sub-theme 1.1. Clean-up
Some focus group participants specifically noted that the clean-up required after preparing a meal contributed to a lack of cooking at home. Simply the thought of cleaning the kitchen was frequently described as a deterrent to cooking.
I love the cooking. I don’t like the clean-up. (Caucasian female caregiver, age 50)
Sub-theme 1.2. Time
Many families expressed a desire to regularly cook meals at home but were challenged with adequate time to prepare meals with their families. Lack of time was often related to busy household schedules, including both child and adult activities outside the home, that limited time spent in the kitchen. Some simply perceived the act of cooking in the home to take considerable time.
Time [is a challenge], and just generally a lot of things going on. Some days we might not cook something as elaborate, we might make something that you just have to heat up. (Caucasian female caregiver, age 37)
Sub-theme 1.3. Cooking tools
Most families new to cooking noted that without the necessary cooking tools, it was difficult to prepare recipes. Some shared that when kitchen supplies were unavailable, they felt limited in the types of foods they could prepare. Many caregivers and children mentioned the particular importance of having measuring cups and spoons available when following recipes.
If you have the bare minimum when it comes to kitchen tools and supplies, that could be challenging when it comes to getting the precise measurements. (African American female caregiver, age 41)
Sub-theme 1.4. Food preferences
When cooking for multiple household members, some focus group participants expressed frustration with accommodating various food preferences. Many caregivers voiced difficulty finding recipes that all members of the household would agree upon and enjoy. Others seemed discouraged when describing meals they had prepared at home that all household members would not eat.
Sometimes we all like different things, so that’s where it can be hard. Some people don’t like potatoes or my husband [doesn’t like] peas. It’s just hard to find something that everybody likes. (Caucasian female caregiver, age 43)
Theme 2. Class format
Flint Families Cook included 7·5 h of live video instruction from a chef and registered dietitian over 5 weeks. Classes started in the evening at approximately 5:00 PM. While the virtual format of the class offered benefits, the reliance on technology also introduced obstacles.
Sub-theme 2.1. Time and length
Most families expressed appreciation for both the timing of classes, which occurred after regular work hours and during dinnertime, and the length of classes, which seemed appropriate to engage youth and families.
Me and [my daughter] really liked the Zoom classes because as soon as I got home from work, we could just go straight into the cooking class. And she had a few minutes after school to prep whatever was needed. (Caucasian female caregiver, age 42)
Sub-theme 2.2. Multiple class nights
Classes were offered two nights each week, and families were given the option of attending the class that best fit their schedules. Most families appreciated the flexibility in class schedules and noted that multiple class nights prevented unpredictable factors, such as technology malfunctions or schedule conflicts, from causing class absences.
Having the option for two days was really good, because there were days where I could do one day or the other and same thing with my family. For the older participants especially, if you have extracurriculars or anything, I had work some days, it was really good having that flexibility. (Multi-racial male youth, age 17)
Sub-theme 2.3. Engagement
During the COVID-19 pandemic, many children, unable to participate in usual after-school activities, were looking for new ways to spend their time. Most families expressed gratitude for Flint Families Cook, an engaging activity for families during this time that served as a resource for youth and families.
With COVID going on, it gave the kids something to do…It’s pretty awesome for them to have a class that they can focus on besides school, and that they can enjoy. Something that was able to de-stress them, knowing that there’s so much craziness going on with COVID. (African American female caregiver, age 36)
Sub-theme 2.4. Technology
On the other hand, the virtual programme format also presented challenges for some families. Because classes relied on technology, attendance and participation were directly impacted by power outages and disrupted Internet connections. Additionally, many families discussed frustrations with the individual devices used to access the classes, including struggles with viewing the computer screen or hearing instructions during recipe preparation.
Some of the weeks I accessed [the class] on my phone. Some weeks I accessed it on my tablet. The internet service has been kind of spotty back and forth. (African American female caregiver, age 57)
Sub-theme 2.5. Class pace
Many caregivers further mentioned that the class pace was not suitable for all families and should be addressed. Some shared that the chef moved through the recipes too quickly and requested that the class pace be slowed. Others suggested stratifying classes in accordance with household cooking experience to help keep all participants moving through the class at the same pace.
There was a couple of times when [the chef] got a little bit ahead of us. So, we were trying to catch up. (Caucasian male caregiver, age 52)
Sub-theme 2.6. Socialisation
Caregivers and children shared that the class format limited socialisation between families. Many caregivers noted that youth, with a special interest in cooking, might have preferred cooking with other children in the class. Some participants also noted that it was difficult to connect with other families during the virtual classes when many had their microphones muted or screens hidden.
I don’t think we really connected with the other families… just because you were at home with your family. And I think if we were to come in and take a cooking class, my child would be more apt to be friendly with the kids. I think just because it’s online, it’s a little bit harder. (Other racial female caregiver, age 40)
Theme 3. Family support
Successfully implementing Flint Families Cook within 104 unique households required consistent investment from caregivers as well as other family members in the home. Focus group participants shared how they supported their family members both before and during the class.
Sub-theme 3.1. Class preparation
Many caregivers discussed how their families engaged in class preparation each week to ensure that they were ready with cooking tools, food and technology. Some shared how they carefully reviewed recipes to determine which cooking utensils and ingredients were required. Others talked specifically about food preparation steps, referred to as ‘prep steps’ within the curriculum. These ‘prep steps’ involved washing, peeling and cutting produce in preparation for classes. Families were encouraged to complete these steps before class to avoid feeling rushed once live instruction started.
I would try to prep beforehand with [my daughter] like, ‘Let’s find all the measuring cups we’re going to need, all the ingredients we’re going to need, what spoons, what bowls’. (Caucasian female caregiver, age 37)
Sub-theme 3.2. Teamwork
Focus group participants shared how family members came together to practise teamwork during the classes. For some, this meant delegating age-appropriate tasks to siblings during recipe preparation, while others shared a genuine feeling of cooperation and support between siblings during class. Members of the household who did not actively participate in cooking often shared in the experience through tasting the prepared meals and offering feedback and support.
The older two [kids] got to do the cutting which I know they liked because they learned new techniques… they took turns a lot and if the older two got to cut, the little one got to mix or measure or things like that. (Other racial female caregiver, age 40)
Sub-theme 3.3. Family bonding
Most families talked about the value of Flint Families Cook in creating a special time for family bonding. Some shared discussions they had with their children while preparing recipes, while others appreciated that this was a dedicated time, free from distractions, for families to simply be together. Some caregivers further mentioned that extended family and friends, who may not live in the home, joined the classes with their children. Various situations were described by participants, including families with shared custody of children who came together to cook; grandparents and other family members who helped caregivers when they were unable to make a class; and youth who invited friends over to cook with them.
It gave us some very dedicated quality time together. It was a time that we were together, intentionally. At home, not work, not school, not video games, not TVs, we’re right here focused on the same task, really working together and creating some memories. (African American female caregiver, age 41)
Theme 4. Provision of food
Flint Families Cook was introduced while grocery store shelves remained empty and food supplies were scarce. Flint Fresh, a food aggregation space for local farmers with mobile food delivery services, partnered with the programme to provide families with ingredients to prepare the class recipes each week. During focus group discussions, it was clear that this part of the programme was critical to its success.
Sub-theme 4.1. Delivery
Families spoke highly of Flint Fresh, with noted comments about positive experiences with the delivery service. Focus group participants appreciated the convenience of receiving food boxes at their homes and had pleasant experiences with the delivery drivers.
The delivery people were really good. They would call me at work and say, ‘Hey, we’re getting ready to come to your house. Is it okay, is there anybody home?’ So, that was nice that I didn’t have food sitting out on my porch getting yucky because of the heat. (Caucasian female caregiver, age 43)
Sub-theme 4.2. Quality and packaging
Participating families noted that the quality and packaging of the food in the ingredient box exceeded their expectations. Families were impressed with the dry ingredients in vacuum-sealed packages, fresh produce and generous portions of food provided in their ingredient boxes.
The boxes were good, a great setup. We were here to bring it in right away and put it away. And there was enough to make the meal and maybe have a little bit extra. I thought all of the packaging was well done, and all the food was fresh and healthy and didn’t have anything that was over-ripe or bad or anything like that. (Caucasian female caregiver, age 42)
Sub-theme 4.3. Child excitement
Many caregivers shared that simply receiving the ingredient box each week elicited excitement from children. Some children talked about anxiously awaiting the arrival of the ingredient boxes to see what was inside, while many caregivers shared that the boxes motivated children to want to cook. Several caregivers noted that the ingredient boxes were the highlight of the programme for their children.
It was exciting because it felt like a Christmas gift that you were waiting to open every single week…we were so excited to see what we were going to make. (African American female youth, age 12)
Theme 5. Instruction and learning
Most focus group participants discussed how the classes offered practical culinary and nutrition education as well as activities that encouraged food exploration. Through the preparation of the weekly recipes with the chef and nutrition education lessons led by the registered dietitian, most families felt they had learned how to identify and create healthy meals.
Sub-theme 5.1. Cooking skills
Children and adults shared that the programme taught or improved their cooking skills. Many participants learned proper knife skills and how to measure recipe ingredients. Several children expressed improved confidence in their cooking abilities, while caregivers shared how they feel more comfortable with their children cooking at home because of their growth during the programme.
[My daughter] definitely learned how to cut, because that was something I didn’t let her do before. But I’ve seen that she was good at it, and she took her time. So, that was great, and she’s learned how to measure ingredients and to look at the label on the measuring spoons and measuring cups. (Caucasian female caregiver, age 30)
Sub-theme 5.2. Nutrition education
Each class included a nutrition lesson facilitated by a registered dietitian. Nutrition content was directly related to the food group that was featured in recipes each week. Families appreciated the discussions and interactive activities that provided nutrition education for the entire family.
You learn from the chef, but you also learn from [the dietitian]. She broke it down into the different food groups and taught about each food group and why it’s good for your body. I kind of knew some of that stuff too but even I learned things. (Caucasian female caregiver, age 43)
Sub-theme 5.3. Food exploration
The recipes prepared in class featured a variety of healthy ingredients that encouraged exploration among participants. In their ingredient boxes, families were introduced to new fruits, vegetables, whole grains and low-fat dairy products. Some participants tried new ingredients for the first time, while others explored recipe preparation with new foods. Each of the class recipes included healthy substitutions, such as incorporating more servings of vegetables, swapping whole grains in place of refined grains or naturally sweetening recipes with fruit or honey.
[The kids] did get introduced [to] new foods, as well as different alternatives of how we traditionally make them, like the mac and cheese was totally not how we make it, but it was good. Everything, all the recipes were amazing. They put a different light on the actual ingredients and how they turned out, so it’s good to have some alternatives, and they still taste great. (African American female caregiver, age 49)
Sub-theme 5.4. Outlook on cooking
Prior to taking the class, many families aspired to regularly cook meals at home, but most felt that their goals were unrealistic given their lifestyle and skillset. After completing Flint Families Cook, families expressed an improved outlook on cooking. For some, this meant cooking more regularly or intentionally including children in meal preparation. Others spoke about how the class improved their perception of cooking.
I got all kinds of confidence…Before I used to be intimidated by the word ‘cook’ and if anyone ever said, ‘Can you help me prepare this food?’ I’d get nervous about using the stove and measuring and how things would turn out, but ever since we’ve done this class, now I feel like I got guts to do anything. Like to make a whole filet mignon dinner. (Multi-racial male youth, age 17)
Discussion
Flint Families Cook was successful in delivering cooking and nutrition education to families virtually, but perhaps more notable was the sentiment that the programme facilitated family bonding. Consistent with earlier findings related to an in-person parent–child cooking programme(Reference Lavelle and Mooney37), both caregivers and children in the current study enjoyed spending quality time with their families during class. Families spoke about how Flint Families Cook encouraged them to support one another and work as a team. Moreover, some talked about the inclusion of extended family members and friends in the programme. Research has shown that involving family members in shared activities, such as preparing and eating meals together, helps to increase family unity and resilience, particularly during times of significant stress(Reference Gayatri and Irawaty38,Reference Imran, Zeshan and Pervaiz39) . The COVID-19 pandemic deeply affected households with children, as many schools, daycare centres and work locations were impacted by stay-at-home orders(Reference Patrick, Henkhaus and Zickafoose28). Social isolation, fear of illness, economic hardship and reduced psychological supports contributed to worsened mental health for both adults(Reference Patrick, Henkhaus and Zickafoose28) and youth(Reference Gadassi Polack, Sened and Aubé40). Studies conducted during the COVID-19 pandemic reported that youth were less likely to exhibit depressive symptoms when their family maintained consistent routines and shared positive experiences together(Reference Gadassi Polack, Sened and Aubé40,Reference Glynn, Davis and Luby41) . When families gathered in their kitchens each week to cook and share a meal, they were likely protecting one another from adversity inflicted by the pandemic(Reference Gayatri and Irawaty38). Furthermore, while most youth recorded declining quality of life during the pandemic(Reference Ahn42), previous research has suggested that young Flint Families Cook participants experienced improvements in health-related quality of life during the 5-week class(Reference Saxe-Custack, Egan and Sadler43). This is in concurrence with results found in another virtual cooking programme offered to children during the COVID-19 pandemic that reported improvements in child wellbeing upon completion of the programme(Reference Hollywood, Issartel and Gaul44). Although Flint Families Cook was designed to improve cooking and nutrition, the programme offered recurring opportunities for families to connect and work together during a difficult time.
The provision of ingredient boxes, delivered each week by Flint Fresh, was a key feature of Flint Families Cook. While some virtual programmes offer vouchers to subsidise class ingredients(Reference Murad, Alford and Davis20,Reference Leveridge, McGregor and Roche23) , Flint Families Cook was unique in supplying complimentary home-delivered food boxes that included all necessary ingredients. Families praised the convenience of the delivered boxes, especially because of the elevated costs and limited availability of many grocery items during the pandemic(Reference Saxe-Custack, Lofton and Dawson35). Inability to access or afford foods is a noted deterrent to participating in virtual cooking classes(Reference Leveridge, McGregor and Roche23). In addition to increasing programme accessibility, the delivered boxes introduced families to healthy ingredients they otherwise may not have purchased due to lack of familiarity or financial constraints(Reference Rao, Afshin and Singh45,Reference Daniel46) . Both adults and youth discussed how they incorporated many new foods created from these ingredients into their diets, an outcome reported in other virtual cooking programmes(Reference Sommer, Pelletier and Roche24,Reference Cunningham-Sabo and Lohse47,Reference Asigbee, Davis and Markowitz48) .
While participating in Flint Families Cook, each caregiver was responsible for ensuring the successful implementation of the virtual programme within their home. Caregivers made decisions that were appropriate for the unique needs and preferences of their household. Most caregivers spoke about how they prepared their kitchen before each class by assembling cooking equipment, following the food ‘prep steps’, and setting up technology. This pre-class set-up contributed to a positive class experience. Previous research focused on virtual classes has noted that adequate preparation before class was paramount to success(Reference Park, Hwang and Baek25). Many caregivers described how they assigned cooking tasks to family members in accordance with cooking skills and facilitated teamwork to ensure that everyone was involved. In some households, caregivers shared that they stepped back and watched as children led food preparation activities. Overall, caregivers seemed to view their role as guiding children during classes, such as making adjustments to speed up the cooking progress when falling behind the pace of the class or troubleshooting when conflicts arose. In these ways, the virtual format required notable commitment from caregivers. This commitment is unlike in-person family cooking classes that typically involve programme staff who prepare the kitchen space, enforce safety and model techniques to include children in the kitchen, allowing caregivers to focus on cooking with their children(Reference Tørslev, Bjarup Thøgersen and Høstgaard Bonde49,Reference Miller, Kaesberg and Thompson50) . It is unclear; however, whether families who complete in-person cooking classes are successfully able to recreate the cooking environment they experienced during the class in their own homes(Reference Tørslev, Bjarup Thøgersen and Høstgaard Bonde49). For example, after finishing a 6-week family cooking class, most caregivers shared that they had not cooked with their children at home because they were concerned about the additional time and vigilance required to keep their children safe in the kitchen(Reference Maslow, Jones and Morris51). Alternatively, Flint Families Cook families practised cooking together at home each week during class, while programme staff provided assistance and encouragement through Zoom. In this way, Flint Families Cook offered structured and supported household cooking time, which may help families continue cooking together at home after the class.
Focus group participants suggested that Flint Families Cook helped overcome barriers to cooking at home. When asked about cooking habits before the class, many caregivers listed various challenges that prevented them from preparing home-cooked meals. Interestingly, after the 5-week class, families’ perceptions of cooking seemed to shift. Most focus group participants believed that cooking at home, especially with their family, seemed more attainable after engaging in the programme. Previous research focused on in-person family cooking classes supports the current findings. After caregivers cooked with their children, caregivers who were hesitant to include their children in the kitchen learned to recognise how children can help in meaningful ways(Reference Lavelle and Mooney37,Reference Tørslev, Bjarup Thøgersen and Høstgaard Bonde49,Reference Miller, Kaesberg and Thompson50) . Some caregivers remarked that cooking at home seemed easier than their previous conceptions and that they aspired to continue cooking together as a family.
Focus group participants pointed to several ways in which Flint Families Cook helped reframe their perceptions of cooking at home. First, the class provided dedicated cooking time each week, which showed busy families how preparing dinner could fit into their schedule. Additionally, families noted improvements in their cooking skills after taking the class, consistent with findings from other virtual programmes(Reference Herman, Kimmel and Shodahl19–Reference Soltanmammedova, Harner and Hornbeck21,Reference Saxe-Custack and Egan26) , which may increase their efficiency in the kitchen. Adults spoke about learning time-saving tricks from the chef and witnessing their children gain confidence and aptitude in the kitchen. Caregivers often worry that involving children in the kitchen will increase the cooking time(Reference Maslow, Jones and Morris51), but studies have shown that caregivers are more willing to welcome children into the kitchen when they witness their children learning new cooking skills(Reference Tørslev, Bjarup Thøgersen and Høstgaard Bonde49,Reference Saxe-Custack, Goldsworthy and Lofton52) . Lastly, Flint Families Cook helped families that were challenged to create meals that addressed various household food preferences by introducing them to new recipes. Many focus group participants offered positive feedback regarding class recipes, and some shared how they had incorporated recipes into their family meals. Likewise, participants in other virtual and in-person programmes have reported preparing class recipes again at home(Reference Soltanmammedova, Harner and Hornbeck21,Reference Leveridge, McGregor and Roche23,Reference Lavelle and Mooney37) . By holding time and supporting families as they cooked together, most focus group participants felt that Flint Families Cook helped address challenges with cooking at home.
This study contains several strengths and limitations. A strength of this study was the inclusion of caregivers and youth in the focus groups, which allowed researchers to hear various participant perspectives. Further, the design of the current study allowed researchers to capture family experiences during a time of crisis and isolation using online methods. One limitation was the small sample of individuals from one low-income community. Because of this, the results may not be generalisable to other communities. Additionally, there may have been selection bias as families that chose to participate in focus group discussions and provide feedback may have had different experiences than those who chose not to participate. However, participants were candid about programme successes as well as programme challenges and offered thoughtful suggestions for improvements.
Conclusion
In addition to perceived positive impacts on cooking skills and nutrition education, many participants shared that Flint Families Cook encouraged family cohesion and support. Most caregivers felt the programme, which included instruction by a chef and dietitian as well as ingredient box delivery, had important impacts on the emotional health of youth and family resilience. Flint Families Cook, and similar virtual scalable programmes, could broadly reach children and families to support physical and psychosocial health, especially in low-resource communities where such interventions may be most beneficial.
Financial support
Flint Families Cook is generously funded by the Stephanie H. and David A. Spina Family Foundation (no assigned grant number). The funders had no role in the study design, data collection, analysis or interpretation.
Competing interests
None.
Authorship
S.E. led the analysis of the data, led all writing and drafting of the manuscript and participated in data collection. A.S.-C. conceived the study, study design and analysis, participated in data collection and contributed to drafting and revising the manuscript. Both authors have approved the final article.
Ethics of human subject participation
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving research study participants were approved by the Michigan State University Institutional Review Board. Written informed consent was obtained from all subjects.

 Open access
Open access