


Food security is defined by the FAO of the UN as ‘a situation that exists when all people, at all times, have physical, social and economic access to sufficient, safe and nutritious food that meets their dietary needs and food preferences for an active and healthy life’(1). Food security requires available, accessible, stable food sources that are utilised by individuals or households. Household food insecurity (HFI) is an ongoing and worsening public health problem in high-income countries around the world. In Canada, HFI is defined as the inability to acquire or consume a sufficient quantity or quality of food(2). In the USA, the United Kingdom, Australia and Canada, HFI has been seen in rising rates in recent years(Reference Kent, Murray and Penrose3–Reference Rabbitt, Hales and Burke6). Households with children are at particularly high risk of experiencing HFI(Reference Loopstra4,5) .
HFI is well understood globally as a social determinant of health with a strong association with household income(Reference Raphael, Bryant and Mikkonen7,8) . Research evidence is mounting for the associations of negative health outcomes and HFI in high-income countries. In adulthood, cardiometabolic conditions linked to diet, such as diabetes, are associated with HFI(Reference Tait, L’Abbe and Smith9–Reference Seligman, Laraia and Kushel15). HFI is associated with premature mortality(Reference Tarasuk, Cheng and Gundersen16) and the inability to adhere to prescription medication(Reference Men, Gundersen and Urquia17). People experiencing HFI are also more likely to require mental health care services(Reference Men, Gundersen and Urquia17) and experience chronic pain requiring the use of opioids(Reference Men, Fischer and Urquia18). Evidence shows that HFI is linked to increased healthcare costs, exacerbating strains on already over-burdened health systems(Reference Men, Urquia and Tarasuk19–Reference Seligman, Bolger and Guzman25).
Research also points to negative health outcomes associated with HFI experienced during childhood and adolescence, but the long-term impact of HFI during this developmentally sensitive period is not fully understood. There is some evidence examining the impact of HFI on early childhood development and physiological outcomes in children aged 0–5 years, demonstrating that HFI is associated with developmental risks and numerous negative physical health outcomes such as anaemia and chronic illness(Reference Simonovich, Pineros-Leano and Ali26,Reference de Oliveira, de Almeida and Gubert27) . In later years, there is evidence that the mental health of youth may be particularly affected by HFI, with reports of increased depression and other mental health issues(Reference McIntyre, Wu and Kwok28,Reference Men, Elgar and Tarasuk29) . Similar to adults, evidence shows that youth experiencing HFI use health services more frequently and incur higher healthcare costs(Reference Anderson, Clemens and Le30,Reference Clemens, Le and Anderson31) .
Despite the increased risk of HFI in households with children and youth and evidence for its detrimental effects on physical and mental health, a comprehensive synthesis capturing the full breadth of health outcomes is not currently available. This rapid systematic review aims to address this gap and synthesise what is known about the association between exposure to HFI during childhood and/or adolescence in high-income countries and physical and mental health outcomes, using studies with stringent measures of HFI. Understanding the full scope of this issue is critical to support advocacy efforts to increase awareness and influence decision makers to take meaningful policy action to reduce HFI among households with children and youth.
Methods
Study design
This rapid review was completed in collaboration with Canada’s National Collaborating Centre for Methods and Tools’ Rapid Evidence Service(Reference Neil-Sztramko, Belita and Traynor32). The review was not registered. The review was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, with deviations to accommodate the rapid timelines reported below(Reference Page, McKenzie and Bossuyt33). A rapid review approach was used given external time and resource constraints and to allow for review completion during a finite professional development placement opportunity. Previous research has demonstrated that rapid reviews report similar conclusions to full systematic reviews, though often with fewer details(Reference Reynen, Robson and Ivory34).
Information sources and search strategy
A public health librarian supported the development of the search strategy. The search strategy underwent peer review through Ontario’s public health Shared Library Services Partnership(35). The search was conducted in Medline, Embase and PsycInfo databases on October 4, 2023, using terms related to ‘food security’, ‘child’ and ‘youth’. To ensure broad health outcomes were captured by the search, the search was not restricted by terms related to outcomes. The full search strategy is included in Appendix A.
Following de-duplication, all identified references were screened using DistillerSR software, first by title and abstract and then by full text. For title and abstract screening, two independent reviewers screened of a sample of ∼10 % of retrieved references. As > 85 % agreement was achieved, the remaining screening was completed by a single reviewer, consistent with a rapid review timeline. The DistillerSR artificial intelligence re-rank function was used to continually assign predicted relevance scores to references and sort references by highest predicted relevance score. References with a relevance score < 0·8 were automatically excluded and not reviewed by a human reviewer(Reference Burns, Etherington and Cheng-Boivin36). Full-text articles deemed potentially relevant at the title and abstract level were screened for eligibility by a single reviewer and double checked by a second reviewer.
Eligibility criteria
English-language primary studies using a quantitative methodology to assess the relationship between experiencing HFI and a physical or mental health outcome were eligible for inclusion. Grey literature was not included to allow for a rapid review timeline. Systematic reviews were excluded to allow for data extraction directly from primary studies(Reference Pollock, Fernandes, Becker, Higgins, Thomas, Chandler, Cumpston, Li, Page and Welch37). Eligible studies included infants, toddlers, children and adolescents aged 18 years and under. To manage the scope of the review, studies focused on maternal health, including studies of HFI during pregnancy and breastfeeding, were excluded. To maximise the generalisability of review findings, studies focused on children or adolescents with chronic health issues (e.g. examining the effects of HFI on a subset of youth living with existing health conditions, such as renal disease or cystic fibrosis) were also excluded. Across the literature, there is high variability in the methods used to measure HFI across studies(Reference Marques, Reichenheim and de Moraes38). The most well-established tool for measuring HFI is the United States Department of Agriculture’s 18-item Household Food Security Survey Module (HFSSM)(39). This tool has been adapted for use in other national surveys, such as in Canada and South Korea(40,Reference Kim, Hong and Kwon41) , and with specific populations(Reference Ellison, Nguyen and Rabbitt42,Reference Hromi-Fiedler, Bermudez-Millan and Segura-Perez43) . Many studies, however, use 1- or 2-question survey items to determine HFI in participants(Reference Simonovich, Pineros-Leano and Ali26,Reference Hager, Quigg and Black44) . While some advocate for the use of these shorter surveys to reduce respondent burden, questions regarding their sensitivity remain(Reference Webb, Coates and Frongillo45,Reference Carletto, Zezza and Banerjee46) . Studies that measured HFI using a validated survey tool and at least four questions to establish the level of HFI were included(Reference McKechnie, Turrell and Giskes47). HFI measured as a binary, e.g. household food insecure v. household food secure, or as a gradient, e.g. severe, moderate, marginal or no food insecurity, was eligible for inclusion. Any physical or mental health-related outcome was eligible for inclusion; however, studies that only measured outcomes related to body size, such as BMI and overweight/obesity, were excluded, given the need in public health practice to divest from using weight-related outcomes as indicators of health(48). Studies that only examined early childhood development, academic and behaviour-related outcomes were also excluded. Studies conducted in low- and middle-income countries were excluded(49).
Quality assessment
The quality of the included studies was evaluated using the JBI suite of critical appraisal tools(50). According to the critical appraisal results, studies were rated low, moderate or high quality at pre-defined threshold scores. Two reviewers completed the quality assessment independently, and conflicts were resolved through discussion.
Data extraction
Two members of the research team completed data extraction for selected articles independently, and conflicts were resolved through discussion. Data for study design, location, population and outcomes were extracted. Data regarding the measurement of HFI, including the survey tool used, the source of data, thresholds to determine levels of HFI and co-variates used in the analysis, were also extracted. Findings with P < 0·05 were considered statistically significant and extracted; non-significant findings were not recorded in the data table to expedite the rapid review timeline. Given the anticipated heterogeneity of covariates used to conduct analyses in each study, both adjusted and unadjusted estimates of effect were extracted.
Data analysis
Meta-analysis was not planned due to the expected heterogeneity of study outcomes and HFI measures. The health outcomes examined in relation to HFI in the included studies were grouped according to nine categories. Findings of studies that reported on outcomes relevant to more than one category were included in more than one analysis. These categories were general health status (e.g. self or parent ratings of general health, chronic health conditions, use of health services and cortisol levels), early childhood (e.g. infant mortality, failure to thrive, growth, development and caregiver-rated overall health), cardiometabolic health (e.g. blood pressure, cholesterol levels and diabetes or HbA1c levels), asthma, dental caries, mental health (e.g. mental health disorders and symptoms and self-esteem), sleep, dietary outcomes (e.g. calorie, macro- and micronutrient intake) and anaemia. Study findings were summarised descriptively and synthesised narratively. Study quality, sample size and study design were considered in the synthesis and interpretation of the findings. Findings are summarised according to reported analyses, including whether there was a statistically significant association between the outcome(s) of interest and HFI as a binary variable, gradients associated with increased severity of HFI and associations with different threshold levels of HFI.
Results
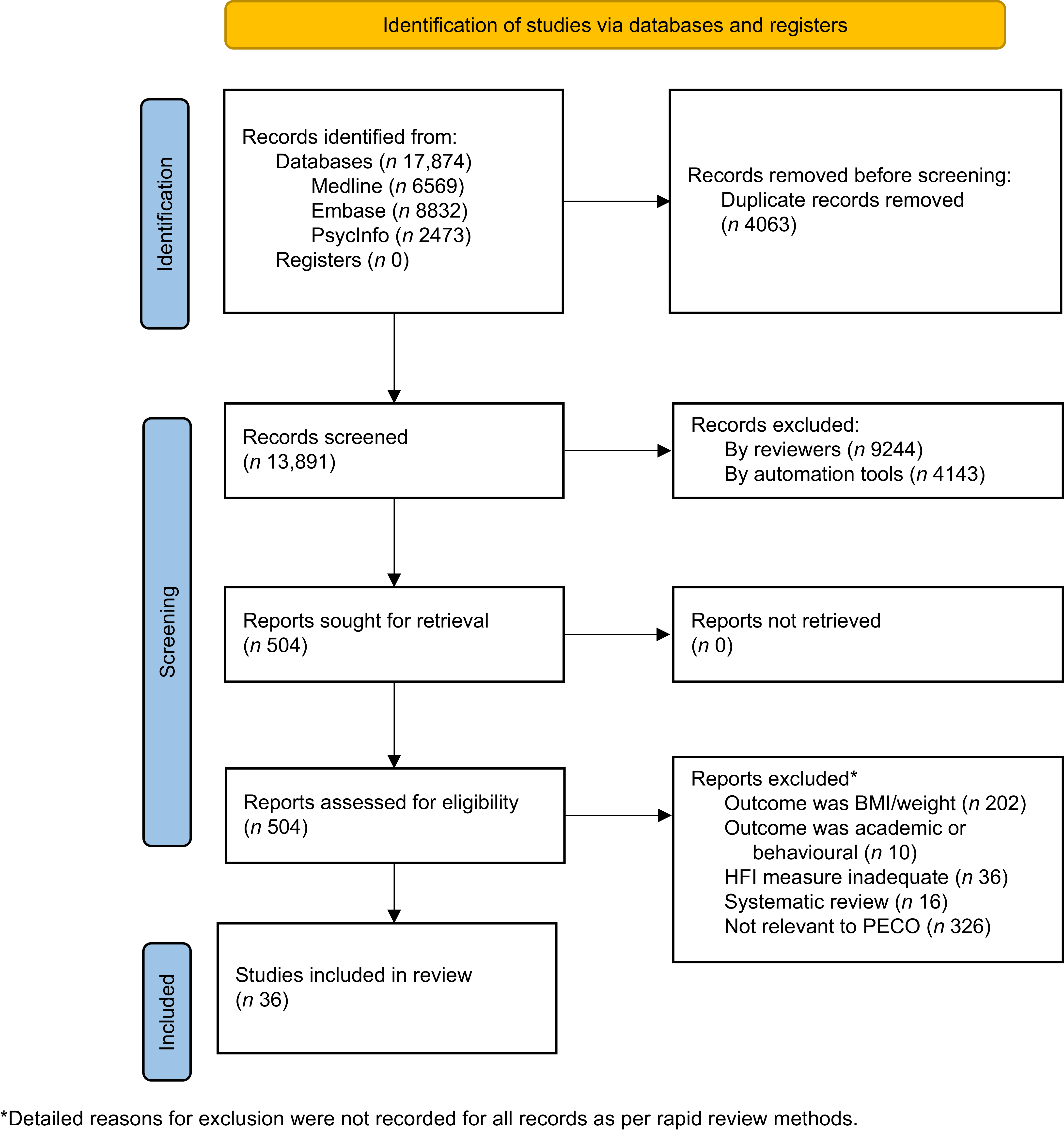
A total of 17 874 records were retrieved after database searching. After removing duplicates, 9748 records were screened by title and abstract, 5605 by a human reviewer and 4143 by AI. The remaining 504 records were assessed at the full-text level by a human review, with thirty-six of these articles deemed eligible for inclusion (Figure 1). Consistent with a rapid review methodology, the reason for exclusion at the full-text level was not recorded for all studies.

Figure 1. PRISMA 2020 flow chart.
Study characteristics
Of the thirty-six included studies, most (n 27, 75 %) were conducted in the United States, followed by Canada (n 7, 19 %)(Reference Anderson, Clemens and Le30,Reference Pirkle, Lucas and Dallaire51–Reference Hutchinson and Tarasuk56) and one study each from France(Reference Arnaud, Lioret and Vandentorren57) and South Korea(Reference Jung, Shin and Lee58) (Table 1). Most studies (n 31, 86 %) included a general or low-income sample of children, while one focused on Urban American Indian/Alaska Native children(Reference Dong, D’Amico and Dickerson69), one on Latinx children(Reference Maldonado, Sotres-Alvarez and Mattei66) and one on Inuit children(Reference Pirkle, Lucas and Dallaire51). Study samples had a wide range of proportions experiencing HFI, from 5·1 % to 86·7 %.
Table 1. Included studies of HFI, grouped by outcomes

FI, food insecurity; FS, food security; HFI, household food insecurity; IRR, incident rate ratio; PR, prevalence ratio; USDA, United States Department of Agriculture; WIC, Special Supplemental Nutrition Program for Women, Infants and Children; NR, Not reported.
* Threshold refers to number of affirmative answers.
Six (17 %) included studies used a cohort design, of which two were conducted prospectively over nearly 10 years(Reference Mangini, Hayward and Dong71,Reference Metallinos-Katsaras, Colchamiro and Edelstein85) , three conducted retrospective analyses of large datasets collected over 8–12 years(Reference Men, Urquia and Tarasuk52–Reference Clemens, Le and Ouédraogo54) and one conducted a retrospective analysis of birth outcomes in a 1-year time period(Reference Sandoval, Jackson and Saleeby59). Five cohort studies were rated as high quality(Reference Clemens, Le and Anderson53,Reference Clemens, Le and Ouédraogo54,Reference Sandoval, Jackson and Saleeby59,Reference Mangini, Hayward and Dong71,Reference Metallinos-Katsaras, Colchamiro and Edelstein85) and one as moderate quality(Reference Men, Urquia and Tarasuk52). Quality assessments are included in online supplementary material, Supplemental Table A2a. The remaining 30 (83 %) studies used a cross-sectional design, and twenty-two were rated as high quality(Reference Anderson, Clemens and Le30,Reference Pirkle, Lucas and Dallaire51,Reference Hutchinson and Tarasuk56,Reference Arnaud, Lioret and Vandentorren57,Reference Tarullo, Tuladhar and Kao60–Reference Cassidy-Vu, Way and Spangler62,Reference Edwards, Schaefer and Murray-Kolb64–Reference South, Palakshappa and Brown70,Reference Bahanan, Singhal and Zhao74,Reference Burke, Martini and Çayır76–Reference Na, Eagleton and Jomaa79,Reference Lee, Kubik and Fulkerson82–Reference Trude, Vedovato and Ali84) , seven as moderate quality(Reference Godrich, Loewen and Blanchet55,Reference Drennen, Coleman and Ettinger de Cuba63,Reference Mangini, Hayward and Zhu72,Reference Angelopoulou, Shanti and Gonzalez73,Reference Hill75,Reference Jun, Cowan and Dodd80,Reference Canter, Roberts and Davis81) and one as low quality(Reference Jung, Shin and Lee58). Quality assessments are included in online supplementary material, Supplemental Table A2b. For most of these studies, methodological quality was enhanced by the use of large, population-level datasets, as well as validated tools for the measurement of HFI; common limitations included self-reported outcome measurements and some incomplete follow-up of study participants.
The most frequently used tool to measure HFI was the Household Food Security Survey Module (HFSSM). The HFSSM is a self-report measure of food access, availability and utilisation, with a primary focus on financial constraints over the last 12 months. The HFSSM was used in 23 (64 %) studies, and a version adapted to Korea was used in one study(Reference Jung, Shin and Lee58). The remaining 12 (33 %) studies all used abbreviated versions of the HFSSM, ranging from four to ten items. Despite using the same tool, some studies stratified participants on a gradient by level of HFI (e.g. food secure, marginal, moderate and severe HFI), while others differentiated participants using a binary variable (food secure v. food insecure). The threshold definition of ‘food secure’ varied, sometimes defined as having zero, one or two affirmative responses to the HFSSM questions.
Study findings
General health status
Overall, six mostly large, high-quality studies examining general health outcomes consistently found poorer outcomes for children experiencing HFI(Reference Pirkle, Lucas and Dallaire51,Reference Men, Urquia and Tarasuk52,Reference Jung, Shin and Lee58–Reference Thomas, Miller and Morrissey61) . Two cross-sectional studies, a large high-quality study of children in the USA(Reference Thomas, Miller and Morrissey61) and a low-quality study of adolescents in South Korea(Reference Jung, Shin and Lee58), found that youth experiencing HFI were more likely to rate their overall health as poor and were more likely to have chronic health conditions(Reference Jung, Shin and Lee58,Reference Thomas, Miller and Morrissey61) . In unadjusted analyses of one small, high-quality cross-sectional study of Inuit children in Northern Quebec, Canada, of which nearly half reported HFI, those who experienced HFI were shorter in stature; however, this effect was not statistically significant when the analysis was adjusted for covariates(Reference Pirkle, Lucas and Dallaire51).
A large moderate-quality cohort study of adolescents in Canada found more emergency department visits for children with any degree of HFI. However, after adjusting for covariates, this effect was only present for moderate or severe HFI(Reference Men, Urquia and Tarasuk52). A smaller, high-quality cohort study looked at the use of health services for infants in the USA and found over twice as many inpatient visits among those experiencing HFI than those in food-secure households (incident rate ratio = 2·4, P = 0·04)(Reference Sandoval, Jackson and Saleeby59).
Two studies also reported on overall stress levels, as measured through self-report(Reference Jung, Shin and Lee58) or hair or salivary cortisol levels(Reference Tarullo, Tuladhar and Kao60). In a low-quality cross-sectional study conducted in South Korea, self-reported stress was higher in adolescent girls in households experiencing HFI than adolescents in food-secure households(Reference Jung, Shin and Lee58). A small, high-quality cross-sectional study of young children conducted in the USA found that children experiencing HFI had higher hair cortisol levels than food-secure peers(Reference Tarullo, Tuladhar and Kao60).
Early childhood outcomes
Findings of three included studies are mixed regarding the association between HFI and early childhood outcomes(Reference Cassidy-Vu, Way and Spangler62–Reference Edwards, Schaefer and Murray-Kolb64). In one high-quality cross-sectional study using county-level data in North Carolina, USA, across all counties in the state, HFI prevalence was strongly associated with the infant mortality rate(Reference Cassidy-Vu, Way and Spangler62). Conversely, in a second high-quality cross-sectional study that analysed data from the National Health and Nutrition Examination Survey (NHANES), no significant associations were found between HFI and the odds of failure to thrive for children(Reference Edwards, Schaefer and Murray-Kolb64). Finally, a moderate-quality cross-sectional study using the Children’s HealthWatch Survey dataset found that caregivers of infants and children aged 0–4 years experiencing HFI had higher odds of poorer caregiver-rated health status compared with food-secure households, but no differences were found in child’s growth or development(Reference Drennen, Coleman and Ettinger de Cuba63).
Cardiometabolic outcomes
Findings for the relationship between HFI and blood pressure were mixed across five high-quality cross-sectional studies(Reference Fulay, Vercammen and Moran65,Reference Maldonado, Sotres-Alvarez and Mattei66,Reference Lee, Scharf and Filipp68–Reference South, Palakshappa and Brown70) . Two large studies of youth in the USA and one small study of American Indian youth found that any level of HFI was associated with higher odds of elevated blood pressure(Reference Lee, Scharf and Filipp68–Reference South, Palakshappa and Brown70). In contrast, a large study of youth in the USA and a smaller study of Hispanic youth found no associations(Reference Fulay, Vercammen and Moran65,Reference Maldonado, Sotres-Alvarez and Mattei66) . The three studies that found an association between HFI and blood pressure all adjusted analyses for child age, sex, race/ethnicity and household income(Reference Lee, Scharf and Filipp68,Reference South, Palakshappa and Brown70) . The two studies that did not find an association adjusted their analyses for additional covariates, such as activity levels, sedentary behaviours, caregiver education and place of birth and household food assistance participation(Reference Fulay, Vercammen and Moran65,Reference Maldonado, Sotres-Alvarez and Mattei66) .
Findings across five cross-sectional studies were also mixed for the association between HFI and cholesterol(Reference Jung, Shin and Lee58,Reference Fulay, Vercammen and Moran65–Reference Tester, Laraia and Leung67,Reference Dong, D’Amico and Dickerson69) . In an analysis that did not adjust for any covariates, a large low-quality study of youth in Korea found that for any level of HFI, blood levels of HDL HDL were lower in girls, and total cholesterol was lower in boys compared with those in food secure households(Reference Jung, Shin and Lee58). A small, high-quality study of youth in the USA found that marginal HFI was associated with higher odds of elevated TAG, TAG:HDL ratio and apo B, but values for those with moderate or severe HFI were not different from food secure households(Reference Tester, Laraia and Leung67). A study of Hispanic youth in the USA found that in unadjusted analyses, moderate or severe HFI was associated with lower HDL and higher TAG. However, this was not seen when the analysis was adjusted for covariates. Additionally, a large study of youth and a small study of American Indian youth in the USA rated high quality found no association between HFI and cholesterol levels(Reference Fulay, Vercammen and Moran65,Reference Dong, D’Amico and Dickerson69) .
Similarly, findings for the association between type 2 diabetes and related markers and HFI were mixed. One large, high-quality cross-sectional study of youth in the USA found that any level of HFI was associated with higher odds of pre-diabetic HbA1c levels after adjusting for child age, sex, race/ethnicity and household income as covariates(Reference Lee, Scharf and Filipp68). However, most studies found no association after adjusting for variables such as activity levels, sedentary behaviours, caregiver education and place of birth and single-parent households(Reference Clemens, Le and Anderson53,Reference Fulay, Vercammen and Moran65,Reference Maldonado, Sotres-Alvarez and Mattei66,Reference Dong, D’Amico and Dickerson69) Three cross-sectional studies, including a large high-quality study in the USA(Reference Fulay, Vercammen and Moran65), a large low-quality study of youth in South Korea(Reference Jung, Shin and Lee58) and a small high-quality study of American Indian youth in the USA, did not find an association between HFI and fasting blood sugar or HbA1c levels(Reference Dong, D’Amico and Dickerson69). In unadjusted analyses, HFI was associated with incident diabetes in a large, high-quality cohort study of children in Canada and fasting blood sugar levels in a small, high-quality cross-sectional study of Hispanic youth in the USA; neither association was found when analyses were adjusted for covariates(Reference Clemens, Le and Anderson53,Reference Maldonado, Sotres-Alvarez and Mattei66) . One study that found no association between HFI and diabetic markers did not adjust for any covariates(Reference Jung, Shin and Lee58).
Asthma
Four studies found an association between HFI and asthma, including two studies of school-aged children that both used data from the Early Childhood Longitudinal Study high-quality cohort study(Reference Mangini, Hayward and Dong71) and the other a moderate quality cross-sectional study(Reference Mangini, Hayward and Zhu72), and a very large high-quality cross-sectional study using NHANES data of children up to age 17(Reference Thomas, Miller and Morrissey61,Reference Mangini, Hayward and Dong71,Reference Mangini, Hayward and Zhu72) . However, a large, high-quality cohort study did not find an association between HFI and incident asthma(Reference Clemens, Le and Ouédraogo54). Each study included many covariates in its analysis; the only study that did not find an association also included household smoking and children’s history of prematurity or intrauterine growth restriction as a covariate(Reference Clemens, Le and Ouédraogo54).
Dental caries
Three cross-sectional studies found an association between HFI and dental caries(Reference Angelopoulou, Shanti and Gonzalez73–Reference Hill75). These include two large studies using NHANES data in the USA, one of which one is high quality(Reference Bahanan, Singhal and Zhao74) and one of moderate quality(Reference Hill75); both noted significant associations when adjusting for covariates. The third was a small moderate quality study conducted in community dental centres in Wisconsin, USA, but did not adjust for covariates in the analysis(Reference Angelopoulou, Shanti and Gonzalez73).
Mental health
Six cross-sectional studies, all using data from large, population-level datasets, explored the association between HFI and mental health outcomes, including anxiety, depressive mood, self-esteem and self-efficacy and use of health services of mental health or substance use(Reference Anderson, Clemens and Le30,Reference Godrich, Loewen and Blanchet55,Reference Jung, Shin and Lee58,Reference Burke, Martini and Çayır76–Reference Poole-Di Salvo, Silver and Stein78) . Two high-quality studies from the USA explored the association between HFI and mental health issues broadly. Data from the 2011–2014 National Health Interview Survey found that the odds of mental disorders, including anxiety, mood, oppositional defiant, attention-deficit hyperactivity and conduct disorders, were higher for children aged 4–17 years with HFI compared with food-secure children(Reference Burke, Martini and Çayır76). The strength of the association increased with the severity of HFI(Reference Burke, Martini and Çayır76). Similarly, a study of data for children aged 12–16 years in the Early Childhood Longitudinal Study initiated in 2007 found increased odds of parent-reported mental health issues, emotional misconduct, peer problems and less optimal pro-social behaviour for any level of HFI compared with no HFI(Reference Poole-Di Salvo, Silver and Stein78). Another high-quality analysis of NHANES data for 12- to 17-year-olds in the USA more specifically explored the odds of anxiety when exposed to HFI and found that HFI was associated with greater odds of experiencing anxiety compared with no HFI(Reference Maynard, Perlman and Kirkpatrick77). A low-quality study explored depressive moods for children aged 10–18 years using the Korea National Health and Nutrition Examination Survey 2012–2019 dataset and found that for girls, there was a statistically significant association with any level of HFI(Reference Jung, Shin and Lee58). Analyses of these large datasets consistently found associations between HFI and poor mental health outcomes.
One study explored the association between HFI and self-esteem and self-efficacy. A moderate-quality study using the Canadian Children’s Lifestyle and School Performance Study II dataset of 10- to 11-year-olds in Nova Scotia, Canada, found that in adjusted analyses, children with any level of HFI had greater odds of low self-esteem and self-efficacy to make healthy choices(Reference Godrich, Loewen and Blanchet55). These findings were not present when the analysis was adjusted for covariates, including the child’s sex, body size, caregiver’s education level, household income and rurality(Reference Godrich, Loewen and Blanchet55).
In terms of the use of mental health services, a high-quality study linking the Canadian Community Health Survey dataset to provincial health records found that the use of mental health or substance use service usage was associated with HFI for children aged 1–17 years; the strength of the association increased with the level of HFI severity(Reference Anderson, Clemens and Le30). Effect sizes were smaller but remained statistically significant when prevalence ratios were adjusted for covariates(Reference Anderson, Clemens and Le30).
Sleep
A small, high-quality cross-sectional study including American Indian adolescents through the Native American Youth Sleep Health and Wellness study(Reference Dong, D’Amico and Dickerson69) found that adolescents with any level of HFI had more sleep disturbances than their food-secure peers(Reference Dong, D’Amico and Dickerson69). Another small, high-quality cross-sectional study examined pre-school aged children in Headstart Preschools in Pennsylvania, USA, and found that preschoolers with any level of HFI had increased odds of poor sleep quality, but this association was not seen when the analysis was adjusted for covariates(Reference Na, Eagleton and Jomaa79).
Diet
In terms of overall diet quality, one large high-quality study in Canada found that children experiencing HFI had lower scores for diet quality(Reference Hutchinson and Tarasuk56). No association between HFI and diet quality was found by three other studies using NHANES data in the USA(Reference Bahanan, Singhal and Zhao74,Reference Jun, Cowan and Dodd80,Reference Lee, Kubik and Fulkerson82) . Findings for daily energy intake were mixed, where two small high-quality studies found that daily energy intake was higher(Reference Trude, Vedovato and Ali84) and lower(Reference Lee, Kubik and Fulkerson82) for children experiencing HFI. Two other studies found no associations or differences between HFI and energy intake(Reference Jun, Cowan and Dodd80,Reference Rossen and Kobernik83) .
Fruit and vegetable intake had the most marked difference for children experiencing HFI and their food-secure peers, but results were still mixed. While four studies (three high quality and one moderate quality) found that fruit and vegetable consumption was lower for children with HFI(Reference Hutchinson and Tarasuk56,Reference Bahanan, Singhal and Zhao74,Reference Canter, Roberts and Davis81,Reference Lee, Kubik and Fulkerson82) , another three studies (two high quality and one moderate quality) found no difference(Reference Jun, Cowan and Dodd80,Reference Rossen and Kobernik83,Reference Trude, Vedovato and Ali84) . Findings for protein and added sugar intake were also mixed. Two high-quality studies found that the proportion of energy intake from protein(Reference Trude, Vedovato and Ali84) and protein from seafood and plant sources(Reference Bahanan, Singhal and Zhao74) was lower for children with HFI, and a low-quality study also found lower protein intake for girls with HFI(Reference Jung, Shin and Lee58). Two other studies, including one high and one moderate quality, did not find a difference in protein intake. Two smaller high-quality studies found differences in sugar intake for children experiencing HFI, specifically in terms of sugar sweetened beverages(Reference Lee, Kubik and Fulkerson82) and added sugars(Reference Trude, Vedovato and Ali84). However, no difference in sugar intake was observed by four other studies(Reference Hutchinson and Tarasuk56,Reference Bahanan, Singhal and Zhao74,Reference Jun, Cowan and Dodd80,Reference Rossen and Kobernik83) . There were no observed differences between children experiencing HFI and their food secure peers for intake of whole grains(Reference Bahanan, Singhal and Zhao74,Reference Jun, Cowan and Dodd80,Reference Rossen and Kobernik83,Reference Trude, Vedovato and Ali84) , Na(Reference Hutchinson and Tarasuk56,Reference Bahanan, Singhal and Zhao74,Reference Jun, Cowan and Dodd80,Reference Rossen and Kobernik83,Reference Trude, Vedovato and Ali84) , fats(Reference Hutchinson and Tarasuk56,Reference Jung, Shin and Lee58,Reference Bahanan, Singhal and Zhao74,Reference Jun, Cowan and Dodd80,Reference Rossen and Kobernik83,Reference Trude, Vedovato and Ali84) or fibre(Reference Hutchinson and Tarasuk56,Reference Jung, Shin and Lee58,Reference Rossen and Kobernik83,Reference Trude, Vedovato and Ali84) .
In terms of micronutrients, two studies reported findings for boys and girls separately(Reference Jung, Shin and Lee58,Reference Jun, Cowan and Dodd80) . A moderate quality study found that for children with HFI, boys had a lower intake of vitamin D, Zn, choline, and Mg, and girls had a lower Ca intake(Reference Jun, Cowan and Dodd80). A low-quality study found that boys had lower vitamin A intake and girls had lower niacin intake when experiencing HFI(Reference Jung, Shin and Lee58). A third moderate quality study found no difference in micronutrient intake for children experiencing HFI(Reference Hutchinson and Tarasuk56).
Anaemia
Relevant to dietary outcomes, four studies reported on the association between HFI and anaemia or markers of Fe deficiency, with mixed findings(Reference Pirkle, Lucas and Dallaire51,Reference Arnaud, Lioret and Vandentorren57,Reference Jun, Cowan and Dodd80,Reference Metallinos-Katsaras, Colchamiro and Edelstein85) . Two analysed large population-level datasets, including a moderate-quality cross-sectional analysis of NHANES data for children aged 1–18 years in the USA(Reference Jun, Cowan and Dodd80) and a high-quality cohort analysis of data for toddlers from a state food assistance program, the Special Supplemental Nutrition Program for Women, Infants, and Children in Massachusetts, USA(Reference Metallinos-Katsaras, Colchamiro and Edelstein85); odds of anaemia were increased in toddlers(Reference Metallinos-Katsaras, Colchamiro and Edelstein85), but this association was not seen across age groups(Reference Jun, Cowan and Dodd80). Additionally, a small, high-quality cross-sectional study that assessed anaemia for children living in shelters while experiencing houselessness in Paris, France found an increased prevalence of anaemia with any level of HFI(Reference Arnaud, Lioret and Vandentorren57). Finally, a small high-quality cross-sectional study of Inuit adolescents in Nunavik, Canada found no association between HFI and anaemia or Fe deficiency(Reference Pirkle, Lucas and Dallaire51).
Discussion
Findings from this review support the hypothesis that exposure to HFI during childhood and/or adolescence is associated with a wide range of negative health outcomes, as evidenced by many high-quality studies. Although there is substantial heterogeneity in terms of HFI measurement and covariate adjustment across studies, findings indicate that HFI is related to negative health outcomes including general health status, asthma, dental caries and mental health. Findings for cardiometabolic health, diet and anaemia are mixed across studies. While challenging to establish causality through observational studies, findings align with many of the Bradford Hill criteria for causal pathways(Reference Shimonovich, Pearce and Thomson86). Particularly, findings are strong, consistent, plausible, show evidence of a clear gradient with increased levels of HFI or ‘dose-response’ and align with evidence for health effects associated with HFI for adults(Reference Gundersen and Ziliak87). Additional high-quality longitudinal studies will provide clarity on the magnitude of these effects. The findings of this review support the importance of taking action to prevent and mitigate the negative health effects of HFI in childhood and adolescence.
In high-income countries, common interventions to address HFI include food banks or food pantries(Reference Loopstra88). Given that many food banks or food pantries rely on donations and volunteer efforts, they are often unable to meet community needs in times of crises, and research evidence has failed to demonstrate that they reduce the prevalence of HFI(Reference Loopstra88). On the other hand, policy interventions that aim to improve the financial circumstances for very low-income households have been shown to reduce HFI prevalence(Reference Loopstra, Dachner and Tarasuk89,Reference Dachner and Tarasuk90) . Effective policy interventions require integration across multiple sectors, including social, economic, health and agriculture, and across all levels of government(Reference Dachner and Tarasuk90). In terms of reducing racial health inequities, a systematic review of structural interventions found that policies that increase income for low-income households had a clearer effect on health outcomes than nutrition programs that focused on access to food(Reference Clark, Cranston and Polin91).
The variation in the measurement of HFI added to the difficulty of comparing results across studies. Varying thresholds for defining food security v. insecurity may explain some heterogeneity in the findings across studies. In instances where a gradient of severity of the outcome of interest according to increasing levels of HFI was reported, findings varied in relation to health outcomes. In some cases, there was a clear gradient effect of increased risk with increasing severity of HFI(Reference Men, Urquia and Tarasuk52,Reference Burke, Martini and Çayır76) , but in others, the observed effect was not necessarily linear(Reference Tester, Laraia and Leung67). Further, there were instances when authors differentiated levels of HFI in the measurement, but findings were grouped and reported as a binary. Within in some of these studies, marginal food insecurity was grouped with food security, but the health impacts of experiencing marginal food insecurity can be significant, and researchers have emphasised the importance of differentiating it from food security(Reference Men, Gundersen and Urquia20,Reference Gregory and Coleman-Jensen92,Reference Cook, Black and Chilton93) . To advance future evidence synthesis for health outcomes and HFI, there is a need for consistent measurement and analysis of HFI within the academic community in this field, particularly in terms of defining threshold categories for levels of HFI.
Covariate adjustment also varied widely among the included studies, adding to the heterogeneity across studies and challenging the synthesis of findings. While adjustment for confounding factors is critical in establishing the independent role of HFI in the health outcome, we emphasise caution against over-adjustment of analyses. When numerous inter-related socioeconomic factors are adjusted for the same analysis, there is potential to over adjust, resulting in attenuation of the true effect of HFI. This is especially true when factors are collinear or intermediaries on the causal pathway between HFI and health outcomes. Careful thought is needed to determine appropriate selection of confounders for adjustment. Differences in approaches to adjustment for confounding across studies may explain some of the heterogeneity in findings. Given the inclusion of studies from several different countries, other factors related to setting and context were also likely to influence study results and affect comparison between studies. Nevertheless, even with the wide variation in covariate adjustment in the studies included in this review, an increased risk of negative health outcomes after being exposed to HFI was demonstrated in most studies.
In literature related to HFI among children and adolescents, it is often cited that adults protect children in the household from food deprivation(Reference McIntyre, Wu and Kwok28,Reference McIntyre, Glanville and Raine94–Reference Hanson and Connor96) . This may partly explain why findings are less clear for physical and dietary-related outcomes but clearer for mental health outcomes. Even if adults in food-insecure households are able to prevent younger members from experiencing food deprivation, children and youth in these households may be highly sensitive to and affected by stressors in the household which could compromise their mental health(Reference Knowles, Rabinowich and Ettinger de Cuba97).
It is important to note that the definition and measurement of HFI in the studies included is specific to income-related constraints. Authors acknowledge that this represents a Western and colonial worldview of HFI, data collection and reporting and is not inclusive of traditional Indigenous views and ways of knowing about food security and food procurement. This is an important consideration in the colonial public health context.
Limitations of this review
There are several important limitations to this rapid systematic review. Heterogeneity in HFI measures and analysis posed a challenge for developing key messaging related to health outcomes. Additionally, using a rapid review approach may increase the risk of bias in the review findings. Modifications to the full systematic review approach include using a single screener to determine eligibility of retrieved studies, with error checking by artificial intelligence. Second reviewers were not blinded to data extraction and quality assessment completed by the first reviewer. The potential bias introduced by these modifications is likely minimal, given the efforts made to pilot a subset of references for screening and data extraction prior to completion by a single reviewer(Reference Garritty, Gartlehner and Kamel98).
Conclusion
HFI continues to pose a major public health challenge, particularly among households with children and youth(Reference Li, St-Germain and Tarasuk99– Reference Thomas, Miller and Morrissey101). While there is wide variability in measurement, this rapid systematic review’s findings indicate important trends related to negative health outcomes associated with experiencing HFI during childhood and adolescence. This review provides evidence for the longer-term negative physical and mental health effects of HFI during this vulnerable life stage. Public health can use the findings of this review to influence policy-level actions by raising awareness about the importance of addressing rising rates of HFI and mitigating the harmful effects of HFI on children and adolescents.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980025101109.
Authorship
E.R. and E.C.C. designed the study, in consultation with S.N-S. and V.T. E.R and V.T. informed question development. E.R. and E.C.C. completed screening, quality assessment and data extraction. E.R. and E.C.C. analysed study results. E.R. and E.C.C. wrote the manuscript in consultation with S.N-S. and V.T. All authors read and approved the final manuscript.
Acknowledgements
The authors would like to acknowledge the NCCMT’s Rapid Evidence Service, particularly Allison Caswell, Aisha Tasawar and Rebecca Blair for their contributions to this review. The authors would also like to acknowledge Tracey Zurich for her contributions to the search strategy for this review.
Financial support
The National Collaborating Centre for Methods and Tools is hosted by McMaster University and funded by the Public Health Agency of Canada. The views expressed herein do not necessarily represent the views of the Public Health Agency of Canada.
The funders had no role in the design of the study, collection, analysis or interpretation of data or in writing the manuscript.
Competing interests
There are no conflicts of interest.
Ethics of human subject participation
Not applicable.




 Open access
Open access