Refine search
Actions for selected content:
59 results
Risk of stroke associated with risperidone in dementia with and without comorbid cardiovascular disease: population-based matched cohort study
-
- Journal:
- The British Journal of Psychiatry , FirstView
- Published online by Cambridge University Press:
- 09 October 2025, pp. 1-7
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Choosing among the long-acting injectable antipsychotics: an evidence-based pragmatic guide
-
- Journal:
- CNS Spectrums / Volume 30 / Issue 1 / 2025
- Published online by Cambridge University Press:
- 18 July 2025, e73
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Chapter 15 - Autism
-
-
- Book:
- The Frith Prescribing Guidelines for People with Intellectual Disability
- Published online:
- 07 November 2024
- Print publication:
- 21 November 2024, pp 209-222
-
- Chapter
- Export citation
Chapter 20 - Children and Adolescents
-
-
- Book:
- The Frith Prescribing Guidelines for People with Intellectual Disability
- Published online:
- 07 November 2024
- Print publication:
- 21 November 2024, pp 297-308
-
- Chapter
- Export citation
Chapter 10 - Aggression and Self-Injurious Behaviour
-
-
- Book:
- The Frith Prescribing Guidelines for People with Intellectual Disability
- Published online:
- 07 November 2024
- Print publication:
- 21 November 2024, pp 131-154
-
- Chapter
- Export citation
Risperidone induced neutropenia in a 75-year-old man
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S724
-
- Article
-
- You have access
- Open access
- Export citation
Less is more
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S468
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Very few research about atrioventricular blocks (AVB) and use of antipsychotic drugs has been made, although it may play an important role in the outcome of any patient affected by psychosis and AVB.
ObjectivesTo describe a case and review clinical data about AVB progression and neuroleptic treatment.
MethodsWe describe a 37 years old inmate male patient who suffered from a first degree AVB and Schizophrenia, being long term treated with neuroleptics (risperidone 9mg/day, switched to paliperidone 9mg/day). Our patient presented very mild symptoms of asthenia and dizziness. An EKG was performed, showing AVB progression to Mobitz Type I1. No structural pathology was assessed by ecocardiography. Holter EKG showed also episodes of third degree AV block. Electrophysiology studies were performed showing a supra-hisian AV Block.
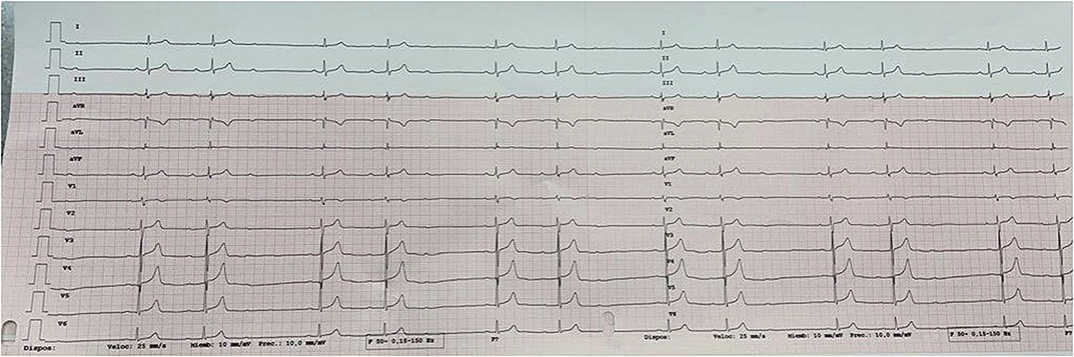 Results
ResultsLower doses of Paliperidone were used (6mg) and maintened until nowadays. Control EKG showed regression to a known first degree AVB.
Being asymptomatic and studies revealing a supra-hisian AVB, no pacemaker was needed.
ConclusionsThere is only a few cases described in scientific literature, and very limited data about AVB and neuroleptic drugs, although it is described as possible side effect using risperidone at higher doses. We suggest monitoring EKG to patients affected by AVB, using high doses of neuroleptic drugs. There is no data available about paliperidone metabolites and a possible progression of AVB.
We suggest more studies are needed to better understand and prevent side effects of neuroleptic drugs.
DisclosureNo significant relationships.

Hyperprolactinemia with antipsychotics and the need for magnetic resonance imaging
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S409
-
- Article
-
- You have access
- Open access
- Export citation
Attention Deficit Hyperactivity Disorder following Hypothalamic Hamartoma Surgery : An unusual manifestation
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S439
-
- Article
-
- You have access
- Open access
- Export citation
P03-47 - The Differences in Producing Cognitive Deficit Between First and Second-Generation Antipsychotics - Our Experiences
-
- Journal:
- European Psychiatry / Volume 25 / Issue S1 / 2010
- Published online by Cambridge University Press:
- 17 April 2020, 25-E1157
-
- Article
-
- You have access
- Export citation
Risperidone in the management of agitation and aggression associated with psychiatric disorders
-
- Journal:
- European Psychiatry / Volume 21 / Issue 1 / January 2006
- Published online by Cambridge University Press:
- 16 April 2020, pp. 21-28
-
- Article
- Export citation
Discriminant cognitive factors in responder and non-responder patients with schizophrenia
-
- Journal:
- European Psychiatry / Volume 14 / Issue 8 / December 1999
- Published online by Cambridge University Press:
- 16 April 2020, pp. 442-450
-
- Article
- Export citation
Risperidone in chronic schizophrenia: a detailed audit, open switch study and two-year follow-up of patients on depot medication
-
- Journal:
- European Psychiatry / Volume 17 / Issue 8 / December 2002
- Published online by Cambridge University Press:
- 16 April 2020, pp. 459-465
-
- Article
- Export citation
Meta-analytic study of the benefits and risks of treating chronic schizophrenia with risperidone or conventional neuroleptics
-
- Journal:
- European Psychiatry / Volume 13 / Issue 6 / September 1998
- Published online by Cambridge University Press:
- 16 April 2020, pp. 310-314
-
- Article
- Export citation
Patients with schizophrenia previously stabilized on conventional depot antipsychotics experience significant clinical improvements following treatment with long-acting risperidone
-
- Journal:
- European Psychiatry / Volume 19 / Issue 4 / June 2004
- Published online by Cambridge University Press:
- 16 April 2020, pp. 219-225
-
- Article
- Export citation
Costs and outcomes of risperidone treatment in schizophrenia in the Czech Republic
-
- Journal:
- European Psychiatry / Volume 17 / Issue 4 / July 2002
- Published online by Cambridge University Press:
- 16 April 2020, pp. 213-221
-
- Article
- Export citation
A comparison of continuous subcutaneous paliperidone infusion and repeated subcutaneous injection of risperidone free-base in rats
-
- Journal:
- European Psychiatry / Volume 25 / Issue 2 / March 2010
- Published online by Cambridge University Press:
- 16 April 2020, pp. 92-100
-
- Article
- Export citation
Establishing remission and good clinical functioning in schizophrenia: Predictors of best outcome with long-term risperidone long-acting injectable treatment
-
- Journal:
- European Psychiatry / Volume 25 / Issue 4 / May 2010
- Published online by Cambridge University Press:
- 16 April 2020, pp. 220-229
-
- Article
- Export citation
A pilot study of the safety and efficacy of amisulpride and risperidone in elderly psychotic patients
-
- Journal:
- European Psychiatry / Volume 24 / Issue 3 / April 2009
- Published online by Cambridge University Press:
- 16 April 2020, pp. 149-153
-
- Article
- Export citation
Two cases of risperidone-induced tardive dyskinesia and a review of the literature
-
- Journal:
- European Psychiatry / Volume 14 / Issue 4 / July 1999
- Published online by Cambridge University Press:
- 16 April 2020, pp. 245-247
-
- Article
- Export citation
