Refine search
Actions for selected content:
79 results
The contaminated blood scandal in England: exploring the social harms experienced by infected and affected individuals
-
- Journal:
- Health Economics, Policy and Law / Volume 20 / Issue 4 / October 2025
- Published online by Cambridge University Press:
- 19 August 2025, pp. 381-396
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A scoping review on the community dividend resulting from testing and treating hepatitis C infection in people living in detention
-
- Journal:
- Epidemiology & Infection / Volume 152 / 2024
- Published online by Cambridge University Press:
- 05 December 2024, e159
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Primary healthcare as a strategy for eliminating hepatitis C: the METRIC toolkit
-
- Journal:
- Primary Health Care Research & Development / Volume 25 / 2024
- Published online by Cambridge University Press:
- 07 November 2024, e61
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Chapter 7 - MicroRNAs Become Medicines
-
- Book:
- Fine-Tuning Life
- Published online:
- 14 June 2024
- Print publication:
- 27 June 2024, pp 175-210
-
- Chapter
- Export citation
Time-to-hepatitis C treatment initiation among people who inject drugs in Melbourne, Australia
-
- Journal:
- Epidemiology & Infection / Volume 151 / 2023
- Published online by Cambridge University Press:
- 09 May 2023, e84
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Chapter 21 - Sexually Transmitted Infections and Pregnancy
- from Section 2 - Specific Issues
-
-
- Book:
- Sex and Pregnancy
- Published online:
- 09 November 2022
- Print publication:
- 27 October 2022, pp 149-164
-
- Chapter
- Export citation
Psychiatrist-led treatment of hepatitis C (HCV) at an opioid agonist treatment (OAT) clinic in Stockholm - enhancing the HCV treatment care cascade
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, pp. S176-S177
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
People who inject drugs (PWID) and opioid agonist treatment (OAT) patients have an increased hepatitis C (HCV) prevalence. Studies among these populations show promising HCV treatment results, which is essential to reach the WHO goal of eliminating HCV as a major public health threat by 2030.
ObjectivesTo introduce psychiatrist-led HCV treatment at an OAT clinic and to investigate HCV treatment results, i.e. sustained virological response at 12 weeks post treatment (SVR12) and numbers of reinfections.
MethodsPrima Maria OAT clinic in Stockholm, provides OAT for 450 patients. The majority have a history of injection drug use. Baseline HCV prevalence (January 2018) was retrospectively investigated through medical charts. In January 2018, psychiatrist-led HCV treatment (with consultation support from infectious diseases specialists) was introduced at the clinic. Prospective treatment results, numbers of reinfections and incidence rates between January 2018 and April 2021 were further investigated.
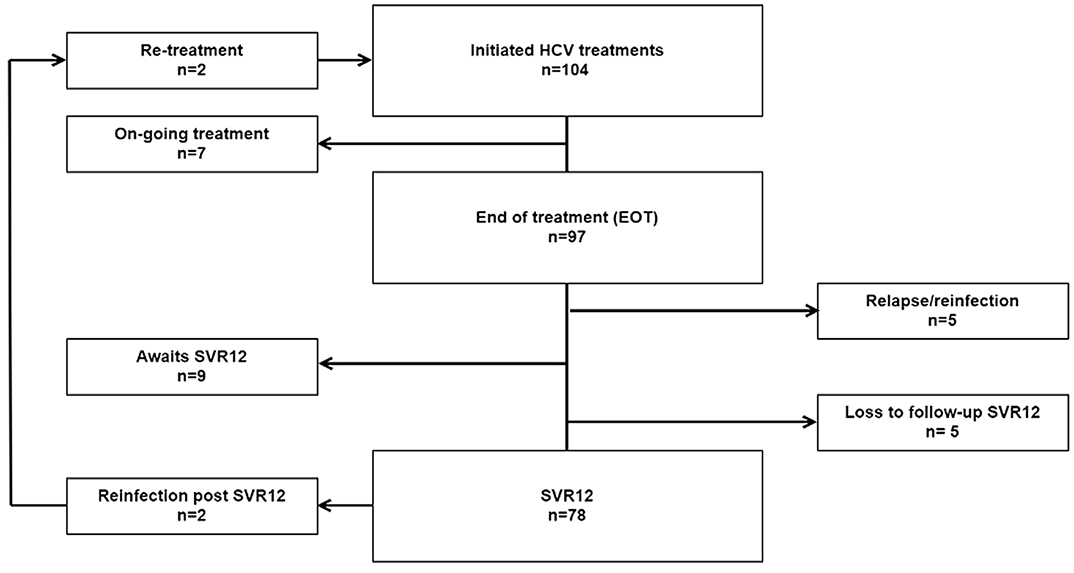
ResultsBaseline data (n=418), showed that 46% were not tested for HCV. Of those tested (n=225), 64% had a chronic HCV infection. By January 2021, 104 HCV treatments were initiated. 97/97 (100%) were HCV RNA negative at end-of-treatment. 78/88 (89%) reached SVR12. Overall, 2 reinfections were noted after SVR12 corresponding to a reinfection rate of 3.5/100 PY. Numbers of HCV treatment did not decrease during the COVID-19 pandemic.
 Conclusions
ConclusionsTo enhance the HCV treatment cascade, targeted HCV diagnosis efforts are needed. Bringing HCV treatment to OAT clinics enhance the HCV care cascade. HCV treatment education for psychiatrists/addiction specialists makes HCV treatment more sustainable, as specifically noted during the COVID-19 pandemic.
DisclosureThis study was partly funded by Gilead Nordic Fellowship 2020. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the poster/manuscript.

Liver function tests in primary care provide a key opportunity to diagnose and engage patients with hepatitis C
-
- Journal:
- Epidemiology & Infection / Volume 150 / 2022
- Published online by Cambridge University Press:
- 27 June 2022, e133
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Real-world monitoring progress towards the elimination of hepatitis C virus in Australia using sentinel surveillance of primary care clinics; an ecological study of hepatitis C virus antibody tests from 2009 to 2019
-
- Journal:
- Epidemiology & Infection / Volume 150 / 2022
- Published online by Cambridge University Press:
- 06 December 2021, e7
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Hepatitis C virus prevalence in Belgium
-
- Journal:
- Experimental Results / Volume 2 / 2021
- Published online by Cambridge University Press:
- 04 October 2021, e29
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Screening for hepatitis C in psychiatric population
-
- Journal:
- European Psychiatry / Volume 64 / Issue S1 / April 2021
- Published online by Cambridge University Press:
- 13 August 2021, pp. S90-S91
-
- Article
-
- You have access
- Open access
- Export citation
Chapter 10 - The Legacies of Belgian Tropical Medicine
-
- Book:
- The Origins of AIDS
- Published online:
- 05 January 2021
- Print publication:
- 21 January 2021, pp 200-232
-
- Chapter
- Export citation
Chapter 9 - The Legacies of French Colonial Medicine
-
- Book:
- The Origins of AIDS
- Published online:
- 05 January 2021
- Print publication:
- 21 January 2021, pp 170-199
-
- Chapter
- Export citation
Chapter 8 - Injections and the Transmission of Viruses
-
- Book:
- The Origins of AIDS
- Published online:
- 05 January 2021
- Print publication:
- 21 January 2021, pp 153-169
-
- Chapter
- Export citation
Maternal hepatitis B or C carrier status and long-term risk for offspring neurological morbidity: a population-based cohort study
-
- Journal:
- Journal of Developmental Origins of Health and Disease / Volume 13 / Issue 1 / February 2022
- Published online by Cambridge University Press:
- 21 January 2021, pp. 115-119
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The transmissibility of hepatitis C virus: a modelling study in Xiamen City, China
-
- Journal:
- Epidemiology & Infection / Volume 148 / 2020
- Published online by Cambridge University Press:
- 25 November 2020, e291
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Numerous outbreaks amongst homeless and injection drug-using populations raise concerns of an evolving syndemic in London, Canada
-
- Journal:
- Epidemiology & Infection / Volume 148 / 2020
- Published online by Cambridge University Press:
- 16 June 2020, e160
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
LO44: Birth cohort hepatitis C screening in an academic emergency department in Canada: preliminary results
-
- Journal:
- Canadian Journal of Emergency Medicine / Volume 22 / Issue S1 / May 2020
- Published online by Cambridge University Press:
- 13 May 2020, p. S23
- Print publication:
- May 2020
-
- Article
-
- You have access
- Export citation
Association of seasonality and serum albumin concentration with vitamin D deficiency in subjects with chronic hepatitis C infection living in a sunny country
-
- Journal:
- Public Health Nutrition / Volume 23 / Issue 7 / May 2020
- Published online by Cambridge University Press:
- 09 March 2020, pp. 1247-1253
-
- Article
-
- You have access
- HTML
- Export citation
Clustering of hepatitis C virus antibody positivity within households and communities in Punjab, India
-
- Journal:
- Epidemiology & Infection / Volume 147 / 2019
- Published online by Cambridge University Press:
- 07 October 2019, e283
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
