Refine search
Actions for selected content:
65 results
Twenty-five year trend in antipsychotic medication prescribing in England: challenges and opportunities
-
- Journal:
- BJPsych Open / Volume 11 / Issue 4 / July 2025
- Published online by Cambridge University Press:
- 16 July 2025, e151
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Clinicians’ perspectives on a primary healthcare intervention to reduce antibiotic prescription for acute lower respiratory tract infections in Barcelona (Spain): a qualitative study
-
- Journal:
- Primary Health Care Research & Development / Volume 26 / 2025
- Published online by Cambridge University Press:
- 04 July 2025, e54
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Chapter 7 - General Aspects of Psychopharmacology
-
-
- Book:
- Fundamentals of Clinical Psychiatry
- Published online:
- 02 January 2025
- Print publication:
- 16 January 2025, pp 50-63
-
- Chapter
- Export citation
Chapter 2 - Prescribing Practice
-
-
- Book:
- The Frith Prescribing Guidelines for People with Intellectual Disability
- Published online:
- 07 November 2024
- Print publication:
- 21 November 2024, pp 13-30
-
- Chapter
- Export citation
Chapter 1 - Intellectual Disability
-
-
- Book:
- The Frith Prescribing Guidelines for People with Intellectual Disability
- Published online:
- 07 November 2024
- Print publication:
- 21 November 2024, pp 1-12
-
- Chapter
- Export citation
The Frith Prescribing Guidelines for People with Intellectual Disability
-
- Published online:
- 07 November 2024
- Print publication:
- 21 November 2024
Can Medical Licensing Boards Swing the Pendulum Towards Judicious Opioid Prescribing Practices?
-
- Journal:
- Journal of Law, Medicine & Ethics / Volume 52 / Issue 3 / Fall 2024
- Published online by Cambridge University Press:
- 16 December 2024, pp. 690-692
- Print publication:
- Fall 2024
-
- Article
- Export citation
Chapter 58 - Public Health and Pandemic Preparedness
- from Section 5 - Patient Management
-
- Book:
- Clinical and Diagnostic Virology
- Published online:
- 11 April 2024
- Print publication:
- 18 April 2024, pp 292-295
-
- Chapter
- Export citation
2 - Prescribing essentials
-
- Book:
- Handbook of Dental Therapeutics
- Published online:
- 23 February 2024
- Print publication:
- 14 March 2024, pp 25-43
-
- Chapter
- Export citation
Medication Use in the Seniors Population: Optimization of Physician Prescribing as a Means of Preventing Drug-related Illness
-
- Journal:
- Canadian Journal on Aging / La Revue canadienne du vieillissement / Volume 16 / Issue S1 / Spring Printemps 1997
- Published online by Cambridge University Press:
- 08 November 2023, pp. 147-161
-
- Article
- Export citation
Evaluation of a new Perinatal Mental Health Service in a University Maternity Hospital
-
- Journal:
- Irish Journal of Psychological Medicine / Volume 40 / Issue 4 / December 2023
- Published online by Cambridge University Press:
- 26 May 2023, pp. 588-591
- Print publication:
- December 2023
-
- Article
- Export citation
Chapter 6 - Use of Medication and Electroconvulsive Therapy in the Management of Violence
- from Section 2 - Medical and Psychological Intervention
-
-
- Book:
- The Prevention and Management of Violence
- Published online:
- 09 May 2023
- Print publication:
- 11 May 2023, pp 76-106
-
- Chapter
- Export citation
Antipsychotic prescribing choices in patients with First Episode Psychosis
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S285
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
As all first line options in treating First Episode Psychosis (FEP) are similarly effective there is a consensus among prescribing guidelines that clinicians and patients should consider side-effect profile as the ‘driver’ of initial choice of antipsychotic. Anecdotally it has been observed that different care teams prescribe particular medications preferentially.
ObjectivesTo evaluate the patterns of antipsychotic prescribing in patients with FEP at the time of initial treatment and over the first year with the Early Intervention Service (EIS).
MethodsMedical records of all patients who had completed 1 year of follow-up with EIS in Sussex Partnership Foundation Trust (n=274) were reviewed. The first antipsychotic prescribed and antipsychotic prescribed at 12-months was recorded alongside initiating care team (EIS, non-EIS community services, inpatient services).
Results99% (n=272) of patients were prescribed an antipsychotic. 46% were initiated by inpatient serves, 40% non-EIS community services and 14% EIS. Aripiprazole, olanzapine, quetiapine and risperidone accounted for 95% of initial prescriptions. Different care teams prescribed antipsychotics preferentially (p=<0.005) (Fig.1). Rates at which initial medication was continued at 12-months varied according to initial prescription (P=<0.05) (Fig.2).
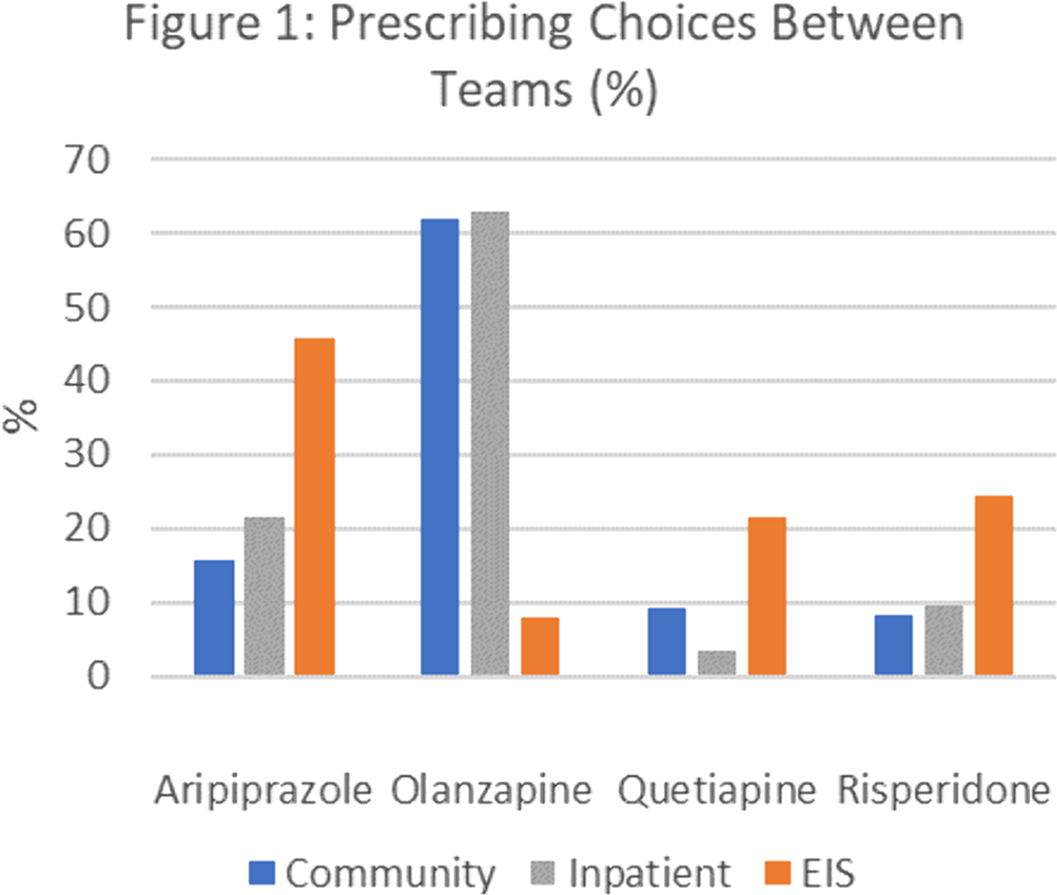
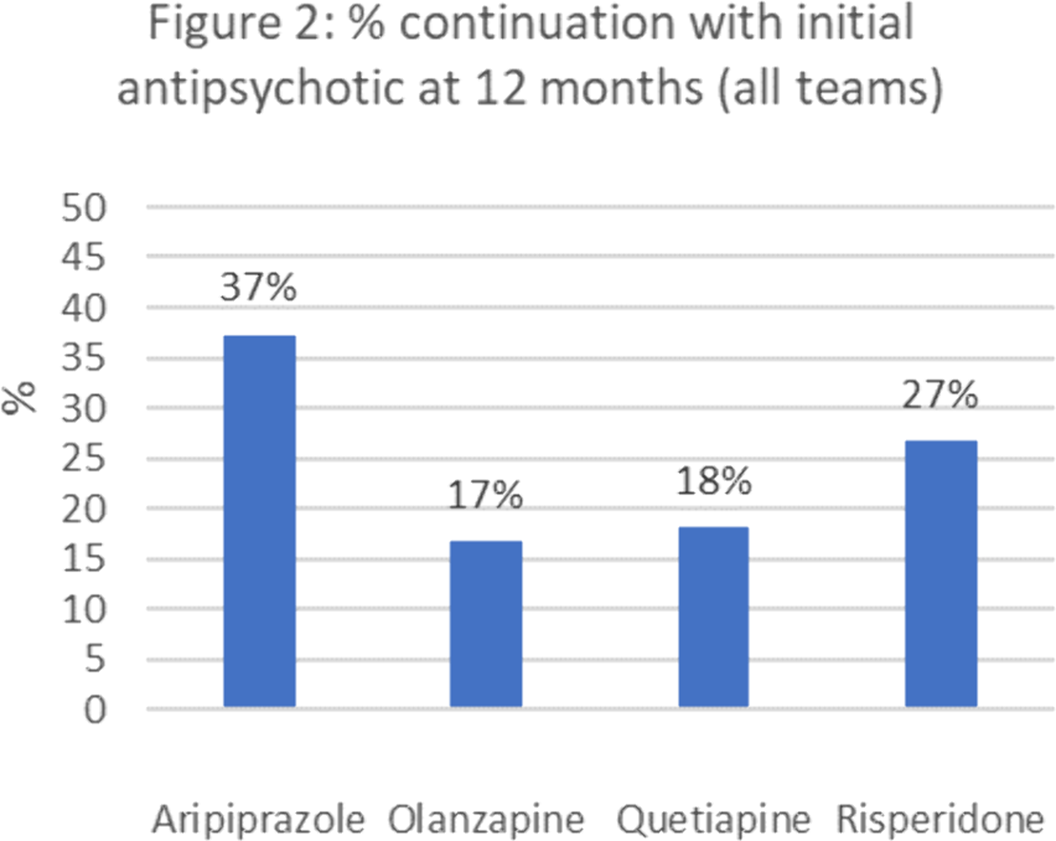 Conclusions
ConclusionsThe frequency that specialist EIS services prescribed aripiprazole as initial treatment contrasts the preference for olanzapine in other services. Olanzapine has a significant metabolic side effect profile, is sedating and was least likely to be continued at 12 months. This raises questions about why non-FEP specialist services prefer olanzapine and whether EIS services can support these services around initial medication choices more likely to be continued throughout the key first year of treatment.
DisclosureNo significant relationships.


Case series: propranolol liquid in the treatment of tachyarrhythmias in neonates and infants: potential for errors
-
- Journal:
- Cardiology in the Young / Volume 33 / Issue 3 / March 2023
- Published online by Cambridge University Press:
- 29 June 2022, pp. 482-484
-
- Article
- Export citation
Will this tablet make me happy again? The contribution of relational prescribing in providing a pragmatic and psychodynamic framework for prescribers
-
- Journal:
- BJPsych Advances / Volume 29 / Issue 4 / July 2023
- Published online by Cambridge University Press:
- 17 June 2022, pp. 265-273
- Print publication:
- July 2023
-
- Article
-
- You have access
- HTML
- Export citation
16 - Antimicrobial Prescribing
-
-
- Book:
- Independent and Supplementary Prescribing
- Published online:
- 23 December 2021
- Print publication:
- 13 January 2022, pp 308-320
-
- Chapter
- Export citation
2 - Non-Medical Prescribing in a Multidisciplinary Team Context
-
-
- Book:
- Independent and Supplementary Prescribing
- Published online:
- 23 December 2021
- Print publication:
- 13 January 2022, pp 8-17
-
- Chapter
- Export citation
10 - Evidence-Based Prescribing
-
-
- Book:
- Independent and Supplementary Prescribing
- Published online:
- 23 December 2021
- Print publication:
- 13 January 2022, pp 172-199
-
- Chapter
- Export citation
COVID-19 pandemic impact on psychotropic prescribing for adults with intellectual disability: an observational study in English specialist community services
-
- Journal:
- BJPsych Open / Volume 8 / Issue 1 / January 2022
- Published online by Cambridge University Press:
- 06 December 2021, e7
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Comparison of paracetamol and diclofenac prescribing preferences for adults in primary care
-
- Journal:
- Primary Health Care Research & Development / Volume 22 / 2021
- Published online by Cambridge University Press:
- 02 December 2021, e78
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
